Approval Date:2007Year. span>03month26day
Revision Date:2014YearOctoberMonth04day
2015Year12month0101day
2019Year08month1919monthmonthmonthmonth family:Arial”>day
2019Year09month0404monthmonthmonthmonth family:Arial”>day
2020YearXXmonthXXmonthmonthmonthmonthmonth family:Arial”>day
Risperidone Tablets Instructions
Please read the instructions carefully and use under medical supervision< span style="font-family:Times New Roman">
Warnings
Increased mortality in older patients with dementia-related psychosis–Older patients with dementia-related psychosis are at increased risk of mortality when using atypical antipsychotics compared with placebo. In 17 placebo-controlled clinical studies in elderly patients with dementia-related psychosis (mean plural treatment duration of 10weeks) found that the risk of death in patients in the drug-treated group wasmore than in the placebo-controlled group. family:Times New Roman”>1.6to1.7 times. In a typical10week controlled clinical study, the mortality rate in the drug-treated group was approximately4.5% and 2.6% in the placebo control group. Although the causes of death vary, most deaths arise from cardiovascular disease (e.g., heart failure, sudden death) or infection (e.g., pneumonia). Risperidone is not approved for the treatment of dementia-related psychosis.
[Drug Name]
Generic Name: Risperidone Tablets
English Name: Risperidone Tablets
Hanyu Pinyin: Lipeitong Pian
[Ingredients]
Active ingredient: Risperidone
Chemical name: 3-[2-[4-(6-fluoro-1,2-benzisoxazol-3-yl)-1-piperidinyl]ethyl]-6,7,8,9-tetrahydro-2-methyl-4H-pyrido[1,2-a]pyrimidin-4-one
Chemical structure formula.
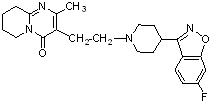
Molecular Formula: C23H27FN4O2
Molecular weight: 410.49
[Properties]
This product is a film-coated tablet, which appears white or off-white after removing the film coating.
[Indications]
1. For the treatment of acute and chronic schizophrenia and various other psychotic states with significant positive symptoms (e.g., hallucinations, delusions, disorganized thinking, hostility, suspicion) and significant negative symptoms (e.g., unresponsiveness, emotional and social indifference, hyposmia). It may also reduce the affective symptoms associated with schizophrenia (e.g., depression, guilt, anxiety). It continues to be clinically effective in maintenance treatment for patients who have been effectively treated in the acute phase.
2. It can be used to treat manic episodes of bipolar disorder, which manifest as elevated mood, exaggerated or irritable, overrated self-esteem, reduced sleep requirements, rapid speech, racing thoughts, distractibility or poor judgment (including disorganized or hyperactive behavior).
[Specifications]
2mg
[dosage]
1.Schizophrenia
Daily11time per day or2times. The recommended starting dose is2times daily1mg, increasing to daily2the next day “font-family:Arial”>times, each time2mg; if tolerated, increase to daily on the third day2timeseachtime, if tolerated. Roman”>3mgtime. Thereafter, this dose may be maintained or further adjusted based on patient response.
The recommended dose range for risperidone is4 per day. Roman”>4to8mg. The effective dose of risperidone ranges from4 to16mg. However, it should be noted that doses above 6 mg daily (according to the twice-a-day dosing regimen) may not provide better efficacy than lower doses Therefore, dose selection should be based on patient response and, in the absence of a definite need, doses greater than 6 mg daily are generally not recommendeddose. The safety of doses above 16 mg dailyhas not been evaluated, therefore, the daily dose of risperidone should not exceed16 mg daily.
Results from clinical trials have shown that the effective dose of risperidone to delay relapse in schizophrenia is a daily2to8mg, and the safety and efficacy of using daily1dose administration. In the trial, the starting dose was1 mgon the first day and increased to daily2mgand on the third day increase to4mg per day. span>, thereafter, this dose may be maintained or further adjusted based on patient response.
Usually, the dose adjustment of risperidone should be slow. The interval between dose adjustments is typically at least one week. When adjusting, the recommended single dose adjustment is 1to~2mg.
The need for and appropriate dose of continued use of this product should be evaluated periodically during treatment. When switching from another antipsychotic to this product, the previously used antipsychotic should be tapered off. The need for continued use of the anti-Parkinsonian medication already in use should be re-evaluated periodically.
2. Manic episode in bipolar disorder
Daily11time daily. The recommended starting dose is1times per day, each time1to2mg. The ideal therapeutic dose for most patients is daily2to6mg, with dose adjustment according to patient needs. The dose adjustment is 1mg daily, with dose adjustment at least at intervals of. family:Times New Roman”>24hours or longer.
The need for continued use of this product and the appropriate dose should be evaluated periodically during the treatment period.
3. Medication for patients with kidney and liver disease
Patients with renal disease have a lower ability to clear the active ingredient of antipsychotic drugs than normal adults, whereas the plasma unbound fraction of risperidone is higher in patients with hepatic disease than normal. concentrations are higher in patients with liver disease than in normal subjects.
The starting dose and maintenance dose should be halved in patients with renal and hepatic disease, and the magnitude and rate of dose adjustment should be reduced. The recommended starting dose is2times per day0.5mgtimes. The dose can be gradually increased to 2times per day, depending on the patient’s needs, each time1to2mg. Dose adjustments should be made at least one week apart. Dose increases and decreases should be in the range of 2times per day0.5mg. Limited clinical experience with the use of this drug in patients with renal and hepatic disease should be used with caution.
[Adverse Reactions]
This product has not been approved for indications other than manic episodes in adults with schizophrenia and bipolar disorder. The following adverse reactions are derived from the information in the original drug insert.
The most common adverse reactions in clinical trials () ≥5percent and were 2fold) included: Parkinson’s disease, inability to sit still, dystonia, tremor, sedation, dizziness, anxiety, blurred vision, nausea, vomiting, epigastric pain, stomach upset, dyspepsia, diarrhea, hypersalivation, constipation, dry mouth, increased appetite, weight gain, fatigue, rash, nasal congestion, upper respiratory tract infection, nasopharyngitis, and sore throat.
The most common adverse reactions leading to discontinuation in clinical trials (leading to> 1% of adults and/or> 2% of pediatric patients discontinued) include: nausea, drowsiness, sedation vomiting, dizziness, and inability to sit still (see [ADVERSE REACTIONS] for discontinuations due to
The data described in this section are from the clinical trials database, which includes patients who received risperidone adult and pediatric patients with schizophrenia, bipolar mania, and autism, pediatric patients with other psychiatric disorders, and patients with dementia who received single or multiple doses, for a total of 9803cases. Of these 9803cases, there were 2687 patients received risperidone while participating in a double-blind, placebo-controlled trial. Risperidone treatment status and duration varied widely, including (overlapping classifications) double-blind, fixed-dose and variable-dose, placebo- or active-controlled trials and open-phase trials, inpatients and outpatients, and short-term (to 12weeks) and long-term (up to3years) dosing. Safety was assessed by collecting adverse events and performing physical examinations, vital signs, weight, laboratory analysis, and ECG.
Clinical trial experience
Because clinical trials are conducted under a variety of different conditions, the incidence of adverse reactions observed in clinical trials for one drug cannot be directly compared to the incidence in clinical trials for another drug clinical trials and does not reflect the incidence in clinical practice.
Common Adverse Reactions in Double-blind, Placebo-Controlled Clinical Trials —- Schizophrenia
Adults with schizophrenia
Table11 span>listed3items span>4to 8weeks in a double-blind, placebo-controlled trial≥2%ofadverse reactions reported in adult patients with schizophrenia treated with risperidone .
Table1 Double-blind, placebo-controlled trial in≥2%(and greater than the placebo group) of risperidone-treated
Adverse reactions reported in adults with schizophrenia< /span> Percentage of patients reporting adverse reactions Risperidone System/Organ Classification 2~8 mg/day >8~16 mg/< /span>day < strong>placebo Adverse Reactions (N=366) (N=198) (N=225) Heart organ disease < span style="font-family:Arial">Tachycardia 1 3 < span style="font-family:Times New Roman">0 Ocular organ disease Blurred vision 3 1 1 Gastrointestinal Disorders < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" >
Nauseous 9 4 4 Constipation 8 9 =”padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none”> 6 Indigestion 8 =”padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none”> 6 5 Dry mouth 4< /span> 0 1 Abdomen Not suitable 3 1 1 Excessive salivation 2 1 <1 Diarrhea 2 1 Systemic diseases fatigue 3 0 Chest Pain 2 1 Lackluster 2 1 <1 < span style="font-family:Arial">Infectious and Infectious Diseases < span style="font-family:Arial">Nasopharyngitis 3 4 < span style="font-family:Times New Roman">3 Upper respiratory tract infection< 2 3 1 Sinusitis 1 1 Urinary tract infection 1 3 All kinds of checks Elevated blood creatine phosphokinase 1 2 <1 Elevated heart rate <1 2 0 Various musculoskeletal and connective tissue disorders > Back Pain 4 1 1 Joint pain 2 3 <1 < span style="font-family:Arial">Limb pain 2 1 < span style="font-family:Times New Roman">1 All types of neurological disorders Parkinson’s disease* 14 17 8 Sitting in silence Cannot* 10 10 3 calm 5 2 Dizziness 7 4
2 Dystonia* 3 4 2 Shock* 2 3 1 2 > 0 < span style="font-family:Times New Roman">0 psychiatric class Insomnia < /td> 32 25 27 > Anxiety 16 11 > 11 Nasal congestion 4 6 2 Breathing difficulties 1 2 0 Epistaxis <1 2 < strong>Dermal and subcutaneous tissue disorders Rash 1 4 1 Dry skin 1 3 0 < span style="font-family:Arial">Vascular disease Upright hypotension 2 < span style="font-family:Times New Roman">1 0 *
“padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none”>
< p style="text-align: center">1
< p style="text-align: center">1
< p style="text-align: center">2
“padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none”>
2
< p style="text-align: center">0
10
< p>Postural dizziness
< p>Respiratory, thoracic and mediastinal disorders
0
Patients with pediatric schizophrenia
Table2listed in a6week, double-blind, placebo-controlled trial. /span>≥5% ofAdverse reactions reported in pediatric schizophrenia patients treated with risperidone .
Table2 double-blind trials in ≥5%(and greater than the placebo group) in the risperidone-treated
Adverse reactions reported in pediatric patients with schizophrenia< /span> Percentage of patients reporting adverse reactions Risperidone System/Organ Classification 1~3 mg/day 4~6 mg/ >day Placebo Adverse Reactions (N=51) < span style="font-family:Times New Roman">(N=54) Gastrointestinal Disorders Excessive salivation 0
10 2 All types of neurological disorders Calm 12 4 Parkinson’s disease* 16 28 11 > Shock 11 10 > 6 9 10 4 Dizziness 7 14 Dystonia* 2 6 0 Psychiatric Anxiety 7 6 0 *
< p style="text-align: center">(N=55)
< p style="text-align: center">24
< p>Sitting still is not an option*
< p style="text-align: center">2
Common adverse reactions in double-blind, placebo-controlled clinical trials —- Bipolar mania
Adult bipolar manic
Table3listed4items3week, double-blind, placebo-controlled, monotherapy trials in≥2% of risperidone-treated adult bipolar manic patients reported adverse reactions.
Table3 double-blind, placebo-controlled, monotherapy trials in≥2% (and greater than placebo group) of risperidone treated
Adverse reactions reported in adult bipolar manic patients Percentage of patients reporting adverse reactions System/Organ Classification Risperidone Placebo Adverse effects 1~6 mg/day span> (N=424) (N=448) Ocular organ disease < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" >
Blurred vision 2 1 Gastrointestinal Disorders < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" >
Nauseous 5 2 Diarrhea 3 2 Excessive salivation 3 1 Stomach upset 2 <1 Systemic Diseases Fatigue 2 1 All types of neurological disorders > Parkinson’s disease* 25 9 Subdued 4 Sitting in silence Cannot* 9 3 Shock* 6 3 Dizziness 5 Dystonia* 5 1 Sleepy< /p> 2 1 *
11
< p style="text-align: center">6
Table4 lists2items 3week, double-blind, placebo-controlled, adjuvant trial in ≥2%of risperidone-treated adult bipolar manic patients reported adverse reactions.
Table4 Double-blind, placebo-controlled, adjuvant therapy trials in ≥2%< span style="font-family:Arial">(and greater than the placebo group) of risperidone-treated
Adverse reactions reported in adult bipolar manic patients Percentage of patients reporting adverse reactions < /tr> System/Organ Classification Risperidone placebo + < Mind Stabilizer < span style="font-family:Arial">Adverse effects (N=127) (N=126) Heart organ disease > Heart palpitations 2 0 Gastrointestinal Disorders Indigestion 9 8 Nauseating 6 4 Diarrhea 6 4 Saliva Hypersecretion 2 0 Systemic diseases Chest Pain 2 1 Infectious and Infectious Diseases > Urinary tract infection 2 1 All types of neurological disorders Parkinson’s disease* 14 Calm 9 4 Sitting still is not an option* 8 0 Dizziness 7 2 shock 6 2 Sleepy 2 1 < strong>Psychiatric class Anxiety 3 2 Respiratory, thoracic and mediastinal disorders Sore Throat 5 2 cough 2 0 *
+ Mental Stabilizer
4
“padding-top: 2px; padding-left: 7px; padding-bottom: 4px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border- right: none”>
Pediatric bipolar manic patients
Table5is listed in a 3week, double-blind, placebo-controlled trial≥5% of the adverse reactions reported in pediatric bipolar manic patients treated with risperidone.
Table5 Double-blind, placebo-controlled trials in≥5%(and greater than the placebo group) in the risperidone-treated
Adverse reactions reported in pediatric bipolar manic patients Percentage of patients reporting adverse reactions Risperidone System/Organ Classification 0.5~2.5 mg/day 3~ =”font-family:Times New Roman”>6 mg/day Placebo Adverse effects (N=50) < span style="font-family:Times New Roman">(N=61) (N=58) Ocular organ disease > Blurred vision 4 7 0 < span style="font-family:Arial">Gastrointestinal Disorders Upper abdominal pain 16 13 5 Nasty 16< /span> 13 7 Vomiting < span style="font-family:Times New Roman">10 10 5< Diarrhea 8 7 Indigestion 10 3 2 < span style="font-family:Arial">Stomach upset 6 0 2 Systemic Diseases fatigue 18 > 30 3 Metabolic and nutritional disorders Appetite Increase 4 7 2 All types of neurological disorders > Calm 42 56 19 dizziness 16< /span> 13 5 Parkinson’s disease* 6 12 3 Myotonia* 6 0 Sitting Still Can’t* < span style="font-family:Times New Roman">0 8 2 Psychiatric category > Anxiety 0 8 3 Respiratory, thoracic and mediastinal disorders Sore Throat 10 3 5 Dermal and Subcutaneous Tissue Disorders Rash 0 7 < span style="font-family:Times New Roman">2 *
2
5
Common adverse reactions in double-blind, placebo-controlled clinical trials —- Autism
Table6listed2items8week, double-blind, placebo-controlled trial and11week, double-blind, placebo-controlled trial and11 family:Arial”>a6week double-blind, placebo-controlled trialin≥5%of Risperidone-treated adverse reactions reported in autism-associated irritable pediatric patients.
Table6 Double-blind, placebo-controlled trials in≥5%< span style="font-family:Arial">(and greater than the placebo group) of risperidone-treated
Adverse reactions reported in autism-associated irritable pediatric patients Percentage of patients reporting adverse reactions System/Organ Classification 0.5< span style="font-family:Arial">~4.0 mg/day< Placebo Adverse effects < strong>(N=107) (N=115 ) Gastrointestinal Disorders < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" >
Vomiting 20 17 Constipation 17 6 Dry mouth 10 4 Nasty 8 5 Excessive salivation 7 1 Systemic diseases and various reactions at the site of administration Fatigue 31 9 Fever 16 13 Thirsty 7 4 Infectious and Infectious Diseases > Nasopharyngitis 9 Rhinitis 9 7 Upper respiratory tract infection 8 3 All kinds of checks weight gain < span style="font-family:Times New Roman">8 2 Metabolic and Nutritional Disorders Increased appetite 44 15 > All types of neurological disorders Calm 63 15 > Salivation 12 4 Headache 12 10 > Shock 8 1 Dizziness 8 2 Parkinson’s disease* 8 < span style="font-family:Times New Roman">1 Kidney and urinary tract disorders Lost urine < /td> 16 Respiratory, thoracic and mediastinal disorders cough 17 Nasal overflow 12 < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" > 10 Nasal congestion 10 < td style="padding-top: 2px; padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: none; border-right: none" > 4 < strong>Dermal and Subcutaneous Tissue Disorders Rash 8 < span style="font-family:Times New Roman">5 *
< p style="text-align: center">Risperidone
19
< /td>
< /td>
< /td>
10
< p style="text-align: center">12
Risperidone and/ or paregoric Other adverse reactions observed during clinical trial evaluation of piperidone
The following adverse reactions have also been observed in placebo-controlled, active-controlled, open studies of risperidone in adults and pediatric patients.
Hematologic and lymphatic disorders: anemia, granulocytopenia, neutropenia;
Heart organ disorders: bradycardia, sinus bradycardia, sinus tachycardia, sinus arrhythmia, first degree AV block, left bundle branch block, right bundle branch block, AV block, conduction disorders, electrocardiogramQTinterval prolongation, postural tachycardia syndrome;
Ear and vagus disorders: ear pain, tinnitus, vertigo;
Endocrine system disorders: hyperprolactinemia, urinary glucose detection;
Ocular organ disorders: ocular congestion, ocular discharge, conjunctivitis, ocular rotation, eyelid edema, ocular swelling, crusting at the eyelid margin, dry eye, increased tearing, photophobia, glaucoma, decreased visual acuity, ocular motility disorders;
Gastrointestinal disorders: dysphagia, bulbous hard stools, fecal incontinence, gastritis, gastroenteritis, lip swelling, labyrinthitis, lack of saliva, gastrointestinal gas, swollen tongue, toothache;
Systemic disorders: peripheral edema, thirst, gait disturbance, flu-like illness, concussive edema, edema, chills, unresponsiveness, malaise, chest discomfort, facial edema, malaise, generalized edema, drug withdrawal syndrome, chills in extremities, mood abnormalities, pain opercular pain, sclerosis;
Immune system disorders: drug hypersensitivity reactions, hypersensitivity reactions, tachyphylaxis;
Infectious and Infectious Diseases: infectious pneumonia, influenza, ear infections, viral infections, pharyngitis, tonsillitis, bronchitis, eye infections, local infections, infections, cystitis, cellulitis, otitis media, nail fungal disease, mite dermatitis, bronchopneumonia , respiratory tract infections, tracheobronchitis, chronic otitis media;
All types of tests: elevated body temperature, elevated blood prolactin, elevated alanine aminotransferase,γ- span style=”font-family:Arial”>elevated glutamyl transferase, abnormal ECG, increased eosinophil count, decreased white blood cell count, elevated glucose, decreased hemoglobin, decreased erythrocyte specific volume, decreased body temperature, decreased blood pressure, elevated transaminases, elevated liver enzymes;
Metabolic and nutritional disorders: decreased appetite, irritability, anorexia, elevated blood cholesterol, elevated blood triglycerides, hyperglycemia, hyperinsulinemia;
Various musculoskeletal and connective tissue disorders: joint stiffness, joint swelling, thoracic musculoskeletal pain, musculoskeletal pain, postural abnormalities, myalgia, neck pain, muscle weakness, rhabdomyolysis;
All types of neurological disorders: balance disorders, attention disorders, dysarthria, dysphonia, loss of stimulus response, decreased level of consciousness, dyskinesia, transient ischemic attacks, coordination disorders, cerebrovascular accidents, speech disorders, syncope, loss of consciousness, tactile hypoesthesia, tardive dyskinesia, movement disorders (including tardive dyskinesia, chorea, choreoathetosis, dyskinesia, muscle twitching, myoclonus), cerebral ischemia, cerebrovascular disorders, nerve blocker malignant syndrome, diabetic coma, head tremor, hypersomnia, convulsions (including grand mal convulsions), sensory abnormalities, psychomotor hyperactivity, hyperkinesia, restless legs syndrome, dystonia (including blepharospasm, cervical spasm, anterior arch recoil, facial spasm, hypertonia, laryngospasm, myotonia, coracoacusis, oropharyngeal spasm, lateral arch recoil, spastic laughter, tics of the hands and feet, tongue spasm, and clenching of the teeth), Parkinson’s disease (including abnormal interbrow reflex);
Psychiatric categories: agitation, emotional dullness, blurred states of consciousness, difficulty falling asleep, intermediate easy awakening insomnia, nervous restlessness, sleep disorders, lethargy, decreased libido and lack of sexual pleasure, depression, nightmares;
Renal and urological disorders: enuresis, dyspareunia, dysuria, urinary incontinence;
Reproductive and breast disorders: amenorrhea, gynecomastia, breast overflow, vaginal discharge, menstrual irregularities (including irregular and infrequent menstruation), delayed menstruation, erectile dysfunction, retrograde ejaculation, ejaculatory disorders, ejaculatory failure, sexual dysfunction, breast enlargement, breast discharge, breast discomfort;
Respiratory, thoracic and mediastinal disorders: croup, aspiration pneumonia, sinus congestion, vocal difficulties, coughing, pulmonary congestion, airway congestion, rales, respiratory disorders, hyperventilation, nasal edema;
Dermal and subcutaneous tissue disorders: erythema, skin discoloration, skin lesions, pruritus, skin lesions, erythematous rash, papular rash, generalized rash, maculopapular rash, acne, skin keratosis, seborrheic dermatitis, dandruff, eczema, drug rash, urticaria;
Vascular and lymphatic vessel disorders: hypotension, flushing, hypertension;
Discontinuation due to adverse reactions
Schizophrenia – Adults
In double-blind, placebo-controlled trials, about7%(39/564) of risperidone-treated patients discontinued due to adverse reactions, compared with placebo group was 4%(10/225). Adverse reactions leading to discontinuation in ≥2 patients treated with risperidone::
Table7 Schizophrenia trials resulting in≥2 “font-family:Arial”>adverse reactions in adult patients discontinuing risperidone treatment
|
Risperidone |
|||
|
2~< span style="font-family:Times New Roman">8 mg/day |
< p style="text-align: center">>8~16 mg/day |
Placebo |
|
|
Adverse effects |
(N=366) |
(N=198) |
(N=225) |
|
Dizziness |
1.4% |
1.0% |
0% |
|
Nasty |
1.4% |
0% |
0% |
|
< span style="font-family:Arial">Vomiting |
0.8% |
0% > |
0% |
|
Parkinson’s disease |
0.8% |
0% |
0% |
|
Drowsiness |
0.8% |
0% |
0% |
|
< span style="font-family:Arial">Dystonia |
0.5% |
0% > |
0% |
|
Riptide |
0.5% |
0% |
0% |
|
Abdominal pain |
0.5% |
0% |
0% |
|
Upright hypotension |
0.3% |
0% |
|
|
Sitting still is not an option |
0.3% |
2.0% |
0% < |
In double-blind, placebo-controlled and active-controlled trials, the placebo-treated group1%of patients in the placebo-treated groupand 3.4%of patients in the active control-treated group due to extrapyramidal symptoms (including Parkinson’s disease, sedentary inability, dystonia, and tardive dyskinesia) were discontinued.
Schizophrenia —- Pediatrics
In double-blind, placebo-controlled trials, about 7%(7/106) of risperidone-treated patients discontinued due to adverse reactions, compared to placebo group was4%(2/54). Adverse effects associated with discontinuation in at least1 patient on risperidone therapy included dizziness (2%), drowsiness (1%< span style="font-family:Arial">), sedation (1%), sleepiness (), and span>1%), anxiety (1%1%), balance disorders (1%), hypotension (1%), palpitations (1%).
Bipolar Mania —- Adult
In double-blind, placebo-controlled trials of risperidone monotherapy, about 6%(25/448) of risperidone-treated patients discontinued due to adverse reactions, compared with 5%of patients in the placebo group ((19/424). Adverse reactions leading to discontinuation in risperidone-treated patients include:
Table8 adverse reactions in bipolar mania trials leading to discontinuation in ≥2adverse reactions in adult patients treated with risperidone
|
Risperidone |
|||
|
1~6 mg/day |
Placebo |
||
|
Adverse Reactions |
(N=448) |
(N=424) |
|
|
Parkinson’s disease |
0.4% |
0% |
|
|
Sleepy |
0.2% |
0% |
|
|
Dizziness |
0.2% |
< p style="text-align: center">0% | |
|
Alanine aminotransferase elevation |
0.2% |
0.2% |
|
|
Elevated aspartate aminotransferase |
0.2% |
0.2% |
Bipolar Mania —- Pediatrics
In double-blind, placebo-controlled trials, about12%(13/111) of risperidone-treated patients discontinued due to adverse reactions, compared with placebo group was 7%(4/58). Adverse effects associated with discontinuation in more than1 cases of risperidone-treated pediatric patients included nausea (3%), drowsiness (2%< span style="font-family:Arial">), sedation (2%), and vomiting (). span>2%).
Autism—-Pediatrics
in autism-related irritable pediatric patients2in an 8week placebo-controlled trial (n=156), there were1one risperidone-treated patient discontinued due to an adverse reaction (Parkinson’s disease); in the placebo group there were1patients discontinued due to adverse events.
Dose Dependence of Adverse Events in Clinical Trials
Extrapyramidal symptoms
from adult schizophrenic patients2data from a fixed-dose trial suggest a dose-related effect on extrapyramidal symptoms associated with risperidone treatment.
In comparing4fixed-dose risperidone (2, , 6,10and16 mg/day) of a8week trial in which two methods were used to measure extrapyramidal symptoms (EPS): (1) Parkinson’s scores from the Extrapyramidal Symptom Rating Scale (mean change relative to baseline); and (2)EPS Incidence of spontaneous complaints:
Table9
|
Placebo |
Risperidone 2 mg |
Risperidone 6 mg |
Risperidone 10 mg |
Risperidone 16 mg |
||||
| 16 mg
tr> |
Parkinson’s disease |
1.2 |
0.9 > |
1.8 |
2.4 |
2.4 |
2.6 |
|
|
EPSincidence< /p> |
13% |
17% |
21% |
21% |
35% |
In comparing5 fixed doses of risperidone (1,4,8,12and16 mg/day) of one8week trial used a similar approach to measure extrapyramidal symptoms (EPS)
Table10
|
Risperidone 1 mg |
Risperidone 4 mg |
Risperidone 8 mg |
Risperidone 12 mg |
Risperidone 16 mg |
||||
| 16 mg
tr> |
Parkinson’s disease |
0.6 |
1.7 > |
2.4 |
2.9 |
2.9 |
4.1 |
|
|
EPSincidence< /p> |
7% |
12% |
17% |
18% |
20% |
Dystonia
Class Effect: In the days prior to treatment, susceptible patients may experience symptoms of dystonia, a prolonged period of abnormal contraction of muscle groups. Symptoms of dystonia include spasm of the neck muscles, which may sometimes progress to a sense of throat constriction, dysphagia, dyspnea and/ or tongue protrusion. Although such symptoms may also occur at low doses, they occur with greater frequency and severity with strong, high-dose first-generation antipsychotic therapy. An elevated risk of acute dystonia was observed in men and in younger age groups.
Other Adverse Reactions
For dose correlation of adverse events, adverse event data extracted from a side effect checklist from a large study comparing5 fixed-dose risperidone (1) family:Arial”>,4,,8,12and16 mg/day). A Cochran-Armitagetest for trends in such data revealed a positive trend for the following adverse reactions (p <0.05): drowsiness, visual abnormalities, dizziness, palpitations, weight gain, erectile dysfunction, ejaculatory dysfunction, sexual dysfunction, and Skin discoloration.
Weight change
Weight gain was observed in short-term, controlled trials and long-term uncontrolled studies in adult and pediatric patients( >see [Caution] ).
Changes in ECG parameters
For the pooled placebo-controlled trials in adults a between-group comparison showed that in ECG parameters (including< span style="font-family:Times New Roman">QT, QTc, PRinterval and heart rate) No statistically significant differences were seen between risperidone and placebo with respect to mean change relative to baseline. When all risperidone doses in randomized controlled trials for several indications were pooled, the mean increase in heart rate was 1beat per minute, whereas in the placebo group Patients showed no change. In short-term trials in schizophrenia, compared with placebo, higher doses of risperidone (8to16 mg/day) correlated with a higher average increase in heart rate (4to6times). In pooled placebo-controlled trials of adult patients with acute mania, there was a small reduction in mean heart rate, which was similar in all treatment groups.
In children and adolescents with autism (5to16years) in 2placebo-controlled trials, the mean change in heart rate in the risperidone group was increased by 8.4 beats per minute in the risperidone group compared with an increase of 8.4 beats per minute in the placebo group, compared with an increase of 6.5 beats. No other significant changes in ECG parameters were seen.
In acutely manic children and adolescents (10to17years) in a placebo-controlled trial, no significant changes in ECG parameters were seen, and only a transient increase in pulse rate occurred in the risperidone group (per minute<6times). In adolescents with schizophrenia (13to17years old)2years old2years old family:Arial”>controlled trials, ECG parameters between or within treatment groups over time (including correctedQT interval) did not show clinically meaningful changes.
Post-marketing experience
In Risperidone and/ or paliperidone during post-approval use, the following adverse reactions were identified. Because such reactions were spontaneously reported from an unknown size group, it was not always possible to reliably estimate the frequency of adverse reactions or to determine a causal relationship with drug exposure. Such adverse reactions include: alopecia, tachyphylaxis, angioedema, atrial fibrillation, cardiopulmonary arrest, diabetic ketoacidosis, taste disturbance, hypoglycemia, hypothermia, intestinal occlusion, dysregulation of antidiuretic hormone secretion, intestinal obstruction, jaundice, mania, pancreatitis, pituitary adenoma, precocious puberty, pulmonary embolism,QTinterval prolongation, sleep apnea syndrome, sudden death, thrombocytopenia, thrombotic thrombocytopenic purpura, urinary retention, water intoxication, granulocyte deficiency, diabetes mellitus, catatonia, sleepwalking disorder, sleep-related eating disorders, intraoperative iris relaxation syndrome, deep vein thrombosis, neonatal drug withdrawal syndrome, and abnormal penile erection.
[Contraindicated]
Discontinued in patients with known hypersensitivity to risperidone, paliperidone, or the excipients in this product.
[Precautions]
This product is not approved for indications other than manic episodes in adults with schizophrenia and bipolar disorder. The following precautions are taken from the original drug insert information.
- Patients with Alzheimer’s disease
1.1Total mortality
for several atypical antipsychotics, including this onea pooled analysis of 17controlled trials of several atypical antipsychotics, including this one, showed an increase in mortality in the atypical antipsychotic group of elderly patients with dementia compared with the placebo group. In placebo-controlled trials with this product in this population, the mortality rate in patients in the product and placebo groups was 4.0%and3.1%. The mean age of patients who died was 86years(range at 67to100yearsof age).
1.2with furosemide Combination
In a placebo-controlled study of Alzheimer’s patients with this product, the mortality rate was higher in patients on risperidone in combination with furosemide than in those on risperidone or furosemide alone patients, respectively, at 7.3% (mean age89 years old, range75to97years), 3.1% (average age84< span style="font-family:Arial">years, range70to< span style="font-family:Times New Roman">96years old) and 4.1% (mean age80years, range67to90 years old). In 4 clinical trials of 2 observed an increase in mortality in patients who combined furosemide and this product.
Although no clear pathophysiologic mechanism has been identified to explain this phenomenon and the causes of death vary among patients, the combined administration of risperidone and furosemide requires careful assessment of risk benefits. In patients taking risperidone in combination with other diuretics, there was no increase in mortality as described above. Because dehydration is an important mortality factor in patients with dementia, it should be avoided as much as possible.
- Cerebrovascular accidents(CAE)
In a study of patients with dementia (mean age85years, range73to97years) in a placebo-controlled study, it was observed that in the risperidone group including adverse cerebrovascular events including death(cerebrovascular accidents and transient ischemic attacks) had a higher incidence than the placebo group.
-
Upright hypotension
Because of its effect onareceptor blockade, upright hypotension may occur, especially during the initial dose adjustment phase of treatment. Clinically significant hypotension has been observed with postmarketing co-administration of antihypertensive drugs. In patients with known cardiovascular disease(such as heart failure, myocardial infarction, conduction abnormalities, dehydration, hypovolemia, or cerebrovascular disease)The product should be used with caution and the dose should be increased gradually according to the recommended dose (see [Dosage and Administration]), and a reduction in dose should be considered if hypotension occurs.
-
Leukopenia, neutropenia, and granulocyte deficiency
Events of leukopenia, neutropenia, and granulocyte deficiency have been reported with antipsychotics, including risperidone. Reports of granulocyte deficiency during postmarketing surveillance were very rare (<1/10,000 patients).
In the first few months of treatment initiation, respond to patients with significantly lowered white blood cells or drug-induced leukopenia/Patients with a history of neutropenia should be monitored and considered for discontinuation of this product once a significant decrease in leukocytes is detected in the absence of other predisposing factors.
Patients with clinically significant neutropenia should be carefully monitored for the presence of fever or other signs or symptoms of infection and treated immediately if these are present. In patients with severe neutropenia (absolute neutrophil count <1×109/L), the product should be discontinued and follow up to monitor the white blood cell count until it returns to normal. -
Venous thromboembolism (VTE)
Cases of venous thromboembolism have been reported with antipsychotic medications. Because risk factors for developing VTE are often present in patients treated with antipsychotics, they should be determined before and during treatment with this product. span>VTEall possible risk factors and preventive measures should be taken before and during this treatment. -
Late onset dyskinesia/Extrapyramidal symptoms (TD/EPS) = “font-family:Arial”>)
Similar to all other drugs with dopamine receptor antagonist properties, this product may cause delayed dyskinesia characterized by rhythmic involuntary movements It is mainly seen in the tongue and face. The development of extrapyramidal symptoms has been reported as a risk factor for the development of tardive dyskinesia, and the risk of tardive dyskinesia is lower with this drug than with other traditional antipsychotics because it is less likely to cause extrapyramidal symptoms. Discontinuation of all antipsychotics should be considered if symptoms of delayed-onset movement disorder occur.
Extrapyramidal symptoms and psychostimulants—Caution is needed in patients receiving a combination of psychostimulants (e.g., methylphenidate) and risperidone, as extrapyramidal symptoms may occur when adjusting one or both drugs. Gradual discontinuation of one or both treatment medications should be considered (see [Drug Interactions]).
-
Nerve blocker malignant syndrome (NMS)Neural blocker malignant syndrome has been reported with conventional antipsychotics and is characterized by hyperthermia, muscle tonicity, autonomic instability The syndrome is characterized by high fever, muscle tonicity, autonomic instability, altered consciousness, and elevated serum creatine phosphokinase levels, and may include myoglobinuria (rhabdomyolysis) and acute renal failure. All antipsychotics, including this product, should be discontinued at this time.
-
Parkinson’s disease or Lewy body dementia
In patients with Lewy body dementia or Parkinson’s disease, the pros and cons should be weighed when prescribing antipsychotics, including this product, which may increase the risk of neural blockers risk of malignant syndrome. At the same time the above population has increased sensitivity to antipsychotic medications and may experience confusion, slowness, and postural instability with frequent falls in addition to extrapyramidal symptoms.
-
Hyperglycemia and Diabetes Mellitus
Hyperglycemia, diabetes mellitus, and exacerbation of preexisting diabetes have been reported during the use of this product. The inherent high risk of diabetes in schizophrenia and the rising incidence of diabetes in the normal population complicate the assessment of the correlation between atypical antipsychotic use and glucose abnormalities. Based on these complexities, the relationship between atypical antipsychotic use and hyperglycemia-related adverse events cannot be adequately understood, and patients treated with atypical antipsychotics, including this product, should be monitored for hyperglycemia and diabetic symptoms.
-
DyslipidemiaAbnormal changes in lipids have been observed in patients treated with atypical antipsychotics.
-
Weight gain
Significant weight gain has been reported. Weight monitoring should be performed when using this product.
-
Hyperprolactinemiawith antagonistic dopamineD2receptors, prolactin levels can be elevated with this product and can persist during long-term administration. Prolactin levels are elevated to a greater extent with this product than with other antipsychotics.
-
FallsDrowsiness, upright hypotension, motor and sensory instability have been reported with antipsychotics (including this product) that can lead to falls and consequently the occurrence of fractures or other injuries associated with falls. The risk of falls should be assessed at the time of initiation of antipsychotic therapy in patients (especially the elderly) with diseases, conditions, or medications that may exacerbate such effects, and repeatedly in patients receiving long-term antipsychotic therapy.
-
Potential cognitive and motor impairmentDrowsiness is a common adverse effect associated with this treatment, especially when determined by direct patient questioning. This adverse reaction is dose-related, and in studies that used a checklist to detect adverse events, the high-dose group (this product16 mg/day) had 41% of patients reported drowsiness, while the placebo group had16% of patients reported. When detecting adverse events, direct questioning was more sensitive than spontaneous reporting, where this product16 mg/day dose group had< span style="font-family:Times New Roman">8% of patients reported adverse effects drowsiness, while in the placebo group1% of patients reported. Because this product may impair judgment, thinking, or motor skills, patients should not operate dangerous machinery (including driving a motor vehicle) until it is reasonably certain that treatment with this product will not cause adverse effects.
-
Difficulty swallowingEsophageal dysmotility and malabsorption are known to be associated with antipsychotic drug use. Aspiration pneumonia is a common cause of morbidity and mortality in patients with late-onset Alzheimer-type dementia. This and other antipsychotic medications should be used with caution in patients at risk for aspiration pneumonia.
-
Intraoperative iris relaxation syndrome (IFIS)
Use of a drug withα1a- intraoperative iris relaxation syndrome) was observed in patients undergoing cataract surgery with adrenergic receptor antagonist effector drugs (including this product).IFISmay increase the risk of intraoperative and postoperative ocular complications. Patients should inform their ophthalmologist prior to surgery of current or previous use of medications with α1a-adrenoceptor antagonistic effects. The potential benefit of discontinuing α1blocking therapy before cataract surgery has not been determined, and the risks of discontinuing antipsychotic medication must be weighed.
-
QTinterval
As with other antipsychotic drugs, it is important for patients with a history of cardiac arrhythmia, congenital long family:Times New Roman”>QT syndrome, and with patients known to prolongQT. span>interval should be used with caution in combination with drugs known to prolong the QTinterval.
-
Abnormal penile erection
withα-< /span>adrenergic blocking effects have been reported to cause abnormal penile erections. During post-marketing surveillance, abnormal penile erections have been reported with this product.
-
Temperature Regulation
The use of antipsychotics can impair the body’s ability to lower deep body temperature. Appropriate care is recommended for patients using this product when they are in conditions that may elevate deep body temperature (e.g., strenuous exercise, exposure to high temperatures, receiving a combination of anticholinergic drugs, or suffering from dehydration).
-
Antiemetic effect
Antiemetic effects have been observed in preclinical studies with risperidone. This effect, if it occurs in humans, may mask signs and symptoms of certain drug overdoses or diseases such as intestinal obstruction, Reye’s syndrome, and brain tumors.
-
Convulsive seizures
As with other antipsychotics, caution should be exercised when using this product in patients with a history of convulsive seizures or other conditions that would potentially lower the threshold for convulsive seizures.
-
Other
For special doses recommended for elderly patients, patients with hepatic impairment, patients with renal impairment, or patients with dementia, see [Geriatric Use] and [Dosage ] sections.
This product has an effect on activities that require alertness. Therefore, until the patient’s sensitivity to this product is known, it is recommended that the patient should not drive a car or operate machinery during treatment.
Please keep out of the reach of children.
[For Pregnant and Lactating Women]
It is not known whether this product is safe for pregnant women to take.
A study based on US Claimsdatabase retrospective observational cohort study comparing the risk of congenital malformations in live-born infants of women with and without antipsychotic use during early pregnancy. After adjusting for confounding variables available in the database, the risk of congenital malformations was elevated in the risperidone group compared with the unexposed antipsychotic group (relative risk=1.26, 95% CI::1.02~1.56). No biological mechanism has been identified to explain this finding, and no teratogenic effect has been observed in nonclinical studies. Based on the results of this observational study, a causal relationship between in utero exposure to risperidone and congenital malformations cannot yet be established.
Animal studies have shown that risperidone is not directly toxic to reproduction and only some indirect prolactin and central nervous system-mediated effects have been observed.
Fetuses exposed to antipsychotics (including risperidone) in late gestation are at risk of developing extrapyramidal or withdrawal symptoms after birth, the severity of which may vary. These symptoms include agitation, hypertonia, hypotonia, tremor, lethargy, respiratory distress, and feeding disorders.
Use this product during pregnancy only if the benefits outweigh the risks.
Lactation: animal studies have shown that risperidone and9-hydroxy–Risperidone is excreted via animal milk. It has also been shown in human trials to be excreted via breast milk, and therefore women taking this product should not breastfeed.
[For Children]
For schizophrenia, there is a lack ofAdequate clinical experience with children under 15 years of age is lacking.
For manic episodes in bipolar disorder, there is a lack ofAdequate clinical experience with children and adolescents under the age of 18is lacking.
[Geriatric use]
Recommended starting dose is 0.5 mg per. style=”font-family:Arial”>twotimes dailyand the dose may be adjusted according to individual needs. Dose increases can be as high as 0.5mgpertimes daily. family:Times New Roman”>2times until once 1to2mg per day2times daily.
[Drug Interactions]
Pharmacodynamic Interactions
Drugs acting on the central nervous system and alcohol
Given the effect of this product onCNS, caution should be exercised when combining with other CNS drugs or alcohol.
Lvodopa and dopamine agonists
This product may antagonize the effects of levodopa and other dopamine agonists.
Drugs that cause hypotension
Clinically significant hypotension was observed with post-marketing combination of risperidone and antihypertensives.
Psychostimulants
Extrapyramidal symptoms may occur when adjusting one or both drugs in the setting of combined psychostimulant (e.g., methylphenidate) and risperidone (see [Cautions]).ProlongedDrugs for QTinterval
Prescribe both this product and prolongedQTinterval should be used with caution.
Pharmacokinetically Relevant Interactions
Food does not affect the absorption of this product.
Risperidone is mainly absorbed via CYP2D6metabolism and to a lesser extent viaCYP3A4metabolism. Risperidone and its active metabolite 9-hydroxy–Risperidone areP-glycoprotein (P-gp) substrates. Substrates that alterCYP2D6 activity or strongly inhibit/inducedCYP3A4and/oror =”font-family:Times New Roman”>P-gp active substrate that can affect the pharmacokinetics of the antipsychotic active ingredient of risperidone.
PotentCYP2D6Inhibitor
This product is compatible with potentCYP2D6inhibitors may increase plasma concentrations of risperidone alone, but less frequently of the antipsychotic active ingredient of risperidone. Higher doses of potentCYP2D6inhibitors may increase the concentration of the antipsychotic active ingredient of risperidone (e.g., paroxetine, below). When initiating or discontinuing the combination of paroxetine or other potentCYP2D6inhibitors, especially at higher doses, physicians should reevaluate the dose of this product.
CYP3A4and/orP-gpInhibitors,
This product is compatible with the potentCYP3A4and/orP-gp inhibitors in combination can substantially increase the plasma concentration of the antipsychotic active ingredient of risperidone. When initiating or discontinuing the combination of itraconazole or other potentCYP3A4and/orP-gpinhibitors, the physician should reassess the dose of this product.
CYP3A4and/orP-gpInducer
This product is compatible with the potentCYP3A4and/orP-gpinduction agents in combination can decrease the plasma concentration of the antipsychotic active ingredient of risperidone. When initiating or discontinuing the combination of carbamazepine or other potentCYP3A4and/orP-gpinducing agent, the physician should reassess the dose of this product.
Drugs with high protein binding
When this product was co-administered with a drug that is highly protein-bound, no clinically relevant plasma protein replacement occurred with either.
When using combination drugs, read the appropriate instructions for information on metabolic pathways and possible need for dose adjustment.
Pediatric population
Interaction studies have been conducted in adults only. It is not clear how relevant the results of the studies are to pediatric patients.
Examples
Drugs that may cause potential interactions or that do not interact with risperidone are listed below:
Antibacterials:
- Erythromycin, a moderateCYP3A4inhibitor, the pharmacokinetics of risperidone alone and the antipsychotic active ingredient of risperidone were not altered.
-
Rifampin, a potentCYP3A4inducer andP-gpinducing agents that reduce the plasma concentration of the antipsychotic active ingredient of risperidone.
Anticholinesterase drugs:
-
Donepezil and galantamine, both of which areCYP2D6andCYP3A4 >substrates, there were no clinically relevant effects on the pharmacokinetics of risperidone alone and the antipsychotic active ingredient of risperidone.
Antiepileptics:
- Carbamazepine, a potentCYP3A4inducer andP-gp< span style="font-family:Arial">inducing agents, reduced plasma levels of the antipsychotic active ingredient of risperidone.
- Topiramate slightly reduced the bioavailability of risperidone alone, but not of the antipsychotic active ingredient of risperidone. Therefore, the interaction is unlikely to be clinically significant.
-
Risperidone has no clinically relevant effect on the pharmacokinetics of valproic acid or topiramate.
Antifungals:
- Itraconazole, a potentCYP3A4andP-gpinhibitors, when the dose of risperidone is2to 8 mg/day when 200 mg/day dose of itraconazole increased the plasma concentration of the antipsychotic active ingredient of risperidone by approximately70%< span style="font-family:Arial">.
-
Ketoconazole, a potentCYP3A4andP-gpinhibitors,200 mg/daily doses of ketoconazole elevated plasma concentrations of risperidone alone and reduced the plasma concentration of 9-hydroxy–Plasma concentrations of risperidone.
Antipsychotics:
- Phenothiazines, which may elevate plasma concentrations of risperidone alone, but not of the active antipsychotic component of risperidone plasma concentrations.
- Aripiprazole, aCYP2D6andCYP3A4substrate: Risperidone tablets or injection do not affect the overall pharmacokinetics of aripiprazole and its active metabolite, dehydroaripipiprazole.
-
Clozapine: long-term co-administration of risperidone and clozapine may decrease the clearance of risperidone.
Antivirals:
-
Protease inhibitors: no formal study data are available; however, because ritonavir is a potentCYP3A4inhibitors and weakCYP2D6inhibitors, ritonavir and ritonavir-boosted protease inhibitors may increase the concentration of the antipsychotic active ingredient of risperidone.
β-Blockers:
-
Somebeta-blockers may elevate risperidone mono plasma concentrations but not risperidone antipsychotic active ingredient plasma concentrations.
Calcium channel blockers:
-
Verapamil, a moderateCYP3A4inhibitor andP-gp< span style="font-family:Arial">inhibitors, elevated plasma concentrations of risperidone alone and the antipsychotic active ingredient of risperidone.
Gangliosides:
-
Risperidone has no clinically relevant effect on the pharmacokinetics of digoxin.
Diuretics:
-
Furosemide: For increased mortality in Alzheimer’s patients with combined use of furosemide, see [Caution ].
Gastrointestinal Drugs:
-
H2-receptor antagonists: cimetidine and ranitidine, both CYP2D6andCYP3A4weak inhibitors of CYP2D6increased the bioavailability of risperidone alone, but the bioavailability of the antipsychotic active ingredient of risperidone was only slightly increased.
Lithium:
-
Risperidone has no clinically relevant effect on the pharmacokinetics of lithium.
SSRIand tricyclic antidepressants:
- Fluoxetine, a potentCYP2D6inhibitor, elevated plasma concentrations of risperidone alone but less so of the antipsychotic active ingredient of risperidone.
- Paroxetine, a potentCYP2D6inhibitor, elevated the plasma concentration of risperidone alone, however, when the dose was as high as20 mg/day, less elevated plasma concentrations of the antipsychotic active ingredient of risperidone were observed. However, higher doses of paroxetine may increase the concentration of the antipsychotic active ingredient of risperidone.
- Tricyclic antidepressants may elevate plasma concentrations of risperidone alone, but not of the antipsychotic active ingredient of risperidone. Amitriptyline does not affect the pharmacokinetics of risperidone or the antipsychotic active ingredient.
-
Sertraline (a weakly potentCYP2D6inhibitor) and fluvoxamine (a weakCYP3A4< span style="font-family:Arial">inhibitor) at doses as high as 100 mg/day , no clinically meaningful changes in the concentration of the antipsychotic active ingredient of risperidone were induced. However, sertraline or fluvoxamine at doses higher than 100 mg/day can increase the concentration of the antipsychotic active ingredient of risperidone.
Table11 Combined drug effects on the active fraction (risperidone+9-) in healthy subjects or patients with schizophrenia >hydroxy–risperidone)
Summary of Effects of Exposure
Co-medication
Dosing regimen
to the active fraction (risperidone+9-hydroxy–risperidone) (ratio*)
Dosing recommendations for risperidone
Co-medication
Risperidone
AUC
Cmax
enzyme (CYP2D6) inhibitor
Fluoxetine
20 mg/day
2or< span style="font-family:Times New Roman">3 mg per day2 per day. times
1.4
1.5
re-evaluate dosing. May not exceed8 mg/day.
Paroxetine
10 mg/day
4 mg/day
1.3
–
Re-evaluate dosing. May not exceed8 mg/day.
20 mg/day
4 mg/day
1.6
–
40 mg/day >
4 mg/day 1.8
–
>
Enzyme (CYP3A/PgPInducer) Inducer
Carbamazepine
573 ± 168 mg/day
3 mg per day >2times
0.51
0.55
Increase the dose. Do not exceed twice the patient’s usual dose
enzyme (CYP3A) inhibitor
Renitidine
150 mg per day2times
1 mgsingle dose
1.2
1.4
No dose adjustment required.
Cimetidine
400 mg2times daily
>
1 mgSingle dose
1.1
1.3
No Dose adjustment.
Erythromycin<
500 mg4times daily
>
1 mgSingle dose
1.1
0.94 No dose adjustment required.
Other Drugs
Amitriptyline
Amitriptyline
50 mg per day. =”font-family:Times New Roman”>2times
3 mg per day2times
1.2
1.1
No dose adjustment required.
*Variation with respect to the reference value
[Drug overdose]
Signs and symptoms
In the presence of acute overdose symptoms, consider whether there are factors caused by other drug combinations.
In general, the signs and symptoms reported in overdose are due to an extension of its pharmacologic effects, including drowsiness and sedation, tachycardia and hypotension, and extrapyramidal symptoms. Prolonged QTintervals and convulsions have been reported in overdose. Tip-twisting ventricular tachycardia has been reported with excessive doses of this product in combination with paroxetine.
Treatment
For overdose relief, maintain a patent airway, ensure adequate oxygen and good ventilation, and consider administration of activated charcoal and light laxatives, and Cardiovascular monitoring, which includes continuous ECG monitoring, should be performed immediately to detect possible arrhythmias. There is no specific antidote for this product. Therefore, appropriate supportive therapy should be used. Hypotension and circulatory deficit may be corrected by intravenous fluids or by administration of sympathomimetic drugs and other appropriate measures. Anticholinergics should be administered once severe extrapyramidal symptoms are present, and close medical monitoring and supervision should be continued until the patient recovers.
Abuse
The potential abuse of risperidone has not been systematically studied in animals or humans. Although clinical trials have not seen a propensity for foraging behavior, such observations are not systematic and cannot be used to predict postmarketing misuse, diversion, and/or abuse situations. Therefore, patients with a history of substance abuse should be evaluated with caution and such patients should be closely monitored for signs of risperidone misuse or abuse (e.g., emergence of tolerance, dose increases, drug foraging behavior).
Dependence
Potential resistance or somatic dependence to risperidone has not been systematically studied in animals or humans.
[Pharmacologic Toxicology]
Pharmacological effects
Risperidone is a selective monoaminergic antagonist of5HT2receptors,D2receptor,a1anda2receptors andH1receptors with high affinity. It also has antagonistic effects on other receptors, but is weak. It has high affinity for 5HT1C, , 5HT1Dand5HT1Aandhave low to moderate affinity forD1and haloperidol-sensitive< span style="font-family:Symbol">sreceptors with weak affinity for MMreceptors with weak affinity for span>receptor orb11 span>andb2 >Receptor without affinity.
The mechanism by which risperidone, like other drugs used to treat schizophrenia, treats schizophrenia is not known. Its therapeutic effect is thought to be on D2receptors and 5HT2receptor antagonism combined effect. For D2and5HT2 antagonism of receptors other than 5HT2 may be related to the other effects of risperidone.
Toxicological studies
Genotoxicity
RisperidoneAmes test, mouse lymphoma test, in vitro rat hepatocyteDNADNA family:Arial”>repair assay, in vivo mouse micronucleus assay, Drosophila companion recessive lethality assay, and in vitro human lymphocyte or Chinese hamster cell chromosome aberration assay were all negative.
Reproductive toxicity
In three Wistarreproductive toxicity assays in rats (two fertility and early embryonic development toxicity assays and one multigenerational reproductive toxicity assay), oral administration of risperidone0.160.16~5 mg/kg [inmg/m2, the maximum recommended human dose (). span>MRHD) 10mg/day (see [dosage]) of. span style=”font-family:Times New Roman”>0.16~4.8 times], affecting mating behavior, but not fertility. This effect occurred only in female rats, as no effect on mating behavior was observed in fertility and early embryonic development assays administered to males only. In a subchronic toxicity test in Beagledogs, oral administration of risperidone at a dose of0.31~5 mg/kg< span style="font-family:Arial">(in mg/m2metered forMRHDof1.0~16.0fold), sperm viability and concentration decreased, and serum testosterone levels decreased dose-relatedly at the same dose; after discontinuation, serum testosterone levels and sperm parameters could be partially restored, but remained at low levels. No no-effect dose was determined in rats or dogs.
InSDandWistar rat and New Zealand rabbit embryonic–fetal litter developmental toxicity assays in which risperidone was administered orally at doses of0.63~10mg/kg ,0.31~5mg/kg(in mg/m) Roman”>mg/m2, respectivelyMRHDof0.64~9.6times,0.640.640.64 span>~9.6fold), no teratogenic effect was observed. No teratogenic effect was observed.
In three reproductive toxicity tests in rats(two perinatal toxicity tests and one multigenerational reproductive toxicity test)in which risperidone was administered orally at a dose of0.16to< span style="font-family:Times New Roman">5mg/kg(in mg/m2, respectivelyMRHDof0.16~4.8fold) when rats are lactating before4day pup mortality was increased. It is unclear whether these deaths were due to direct effects on fetuses or pups or to maternal effects. A no-effect dose for increased pup mortality in rats was not determined. In a perinatal toxicity trial,2.5 mg/kg (in mg/m2asMRHD). /span>of2.4fold) when Rat pups had increased stillbirths. In a rat cross-fostering assay, toxic effects on fetuses or pups were characterized by a decrease in the number of live pups at birth, an increase in the number of dead pups, and a decrease in the birth weight of pups from the administered dams. In addition, there was an increase in pup mortality on the first day of life in the administered dams, regardless of whether the pups were cross-fostered. Risperidone may have impaired maternal behavior, with reduced body weight gain and survival of pups produced by control animals and raised by dosed dams (lactation day 1~4days). These effects were all at 5 mg/kg (in mg/m2 for MRHD< span style="font-family:Arial">of4.8fold) was observed at the dose.
Risperidone can be transferred to rat pups via the placenta.
Carcinogenicity
Risperidone was given by adulteration in mice and rats respectively. family:Times New Roman”>0.63,2.5,10mg/kg(to< span style="font-family:Times New Roman">mg/kg, respectivelyMRHDof3.2, 14.4, 60.8 times; withmg/m2mice doses wereMRHD of0.32, 1.2,4.8fold The dose in rats was0.8fold of MRHD respectively: Times New Roman”>0.64, 2.4, 9.6fold), with dosing cycles of =”font-family:Times New Roman”>18months and25< span style="font-family:Arial">months. The maximum tolerated dose was not reached in male mice. The results showed statistically significant increases in pituitary adenomas in female mice, pancreatic endocrine adenomas in male rats, and mammary carcinomas in female mice and male and female rats.
Anti-psychotic drugs can cause prolactin levels to be chronically elevated in rodents. Prolactin levels were not measured in the risperidone carcinogenicity test, but in a subchronic toxicity test, oral administration of the same dose of risperidone as in the carcinogenicity test resulted in a dose-dependent increase in prolactin levels in mice and rats, up to 55, respectively. to6fold. Increased incidence of pituitary, endocrine pancreatic, and mammary gland tumors have been found in rodents when other antipsychotics are administered chronically and are thought to be mediated by prolactin. The correlation between the occurrence of prolactin-mediated endocrine tumors in rodents and the risk of human use is unclear.
Other toxicity
Puppies of40week toxicity test in which risperidone was given orally0.31,1.25,5mg/kg/day, a reduction in bone length and density was observed with a no-effect dose of0.31 mg/kg/day. In addition, delayed sexual maturation was observed in both males and females in all dose groups. After a recovery period of 12weeks of discontinuation, the above effects in females did not show or largely did not show reversibility.
In a toxicity test in young rats on 1212to50day-old oral administration of risperidone, reversible learning and memory impairment was observed only in females at a no-effect dose of0.63 mg/kg/day. No effects on neurobehavioral or reproductive development were seen at the highest dose of 1.25 mg/kg/day.
[Pharmacokinetics]
Risperidone is completely absorbed after oral administration and is family:Times New Roman”>1~2hours to peak blood levels, and its absorption is not affected by food, so it can be taken alone or with food. In vivo, risperidone is metabolized by CYP2D6 to CYP2D6. family:Times New Roman”>9-hydroxy–Risperidone, the latter has similar pharmacological effects to Risperidone. Risperidone is associated with9-hydroxy–Risperidone together constitute the antipsychotic active ingredient of this product, and the other metabolic pathway of Risperidone in the body isN dehydrocarbonation. The elimination half-life of risperidone is about 3hours,9-hydroxy––Risperidone and other active metabolites have an elimination half-life of 24 hours. Most patients achieve risperidone homeostasis within 1day after family:Times New Roman”>4to5day to reach9-hydroxy–Risperidone is steady-state, with blood concentrations of risperidone proportional to the administered dose in the therapeutic dose range. It is rapidly distributed in the body with a volume of distribution of 1to~2L/kg, in plasma, risperidone is associated with albumin anda< span style="font-family:Times New Roman">1 acid glycoprotein binding, the plasma protein binding of risperidone was88%, 9-hydroxyl–plasma protein binding of risperidone was77%. After 1week of medication,, Roman”>70% of the drug was excreted in the urine,14% of the drug is excreted via feces, and of the fraction excreted via urine,35to< span style="font-family:Times New Roman">45%for risperidone and 9-hydroxy–risperidone , the rest being inactive metabolites. A single-dose study showed that plasma concentrations of the active ingredient were higher in elderly patients and in patients with renal insufficiency, and that clearance of the active ingredient was reduced by 30% in elderly patients. family:Arial”> and in patients with renal insufficiency60%. Risperidone plasma concentrations were normal in patients with hepatic insufficiency, but the mean increase in the unbound fraction of risperidone in plasma was about 35%. Risperidone,9-hydroxy–Risperidone and other antipsychotic active metabolites have similar pharmacokinetics in children as in adults.
[Storage]
Seal and store.
[Packaging]
Medicinal plastic bottle:30tablets/bottle.
[Expiration date]
12months
[Executive Standard]
[approval number]
2mg:国药准字H20051731
[Drug Marketing Licensee]
Name
Name: Changzhou Four Pharmaceuticals Co.Registered address: Meilongba, south suburb of Changzhou City, Jiangsu Province
Postal Code:213004
[Manufacturer]
Manufacturer: Changzhou Four Pharmaceuticals Co. family:Times New Roman”>
Manufacturing Address: Zhongwu Avenue, Changzhou City, Jiangsu Province567No.
Postal Code:213018
Phone Number:800-8284141
(0519)88804418
Fax Number:(0519)88825678
Web
at:www.czsiyao-pharm.com