Currently, surgery is still the best treatment option for lung cancer, and patients with early-stage lung cancer do not necessarily need adjuvant chemotherapy after surgery. However, unfortunately, a considerable number of patients have already lost the opportunity of surgery when first detected and can only be treated by conservative therapy, such as chemotherapy, radiotherapy, targeted or immunotherapy. However, no matter which method is used, the pathological type of lung cancer needs to be clarified first.
Lung cancer tissue biopsy is an important means to obtain tissue specimens and further define the pathological type. With the application of CT, Endobronchial Ultrasonography (EBUS) and other technologies, lung cancer biopsy techniques have been improved and lung cancer diagnosis and treatment have become more accurate.
Currently, transbronchial lung biopsy (TBLB), CT-guided percutaneous lung aspiration biopsy, and biopsy of metastatic masses (especially enlarged lymph nodes) are the most commonly used biopsy methods in clinical practice. Aspiration (TBNA), mediastinoscopy, and medical thoracoscopy are also commonly used by physicians to obtain tumor pathology. Sometimes, physicians also perform cytology on pleural fluid or bronchial cell lavage to obtain a tumor pathology diagnosis. How do physicians choose to use the appropriate “tools” to successfully obtain tumor tissue for pathologic diagnosis?
I. Transbronchoscopic lung aspiration biopsy
Transbronchoscopic lung aspiration biopsy is appropriate for lesions growing in the central part of the lung. If the tumor is growing within the bronchial lumen, the surgeon can remove the tumor tissue under direct vision; if it is growing outside the lumen, the surgeon will use x-ray guidance to confirm that the biopsy forceps are located in the tumor tissue and then clip the tumor tissue.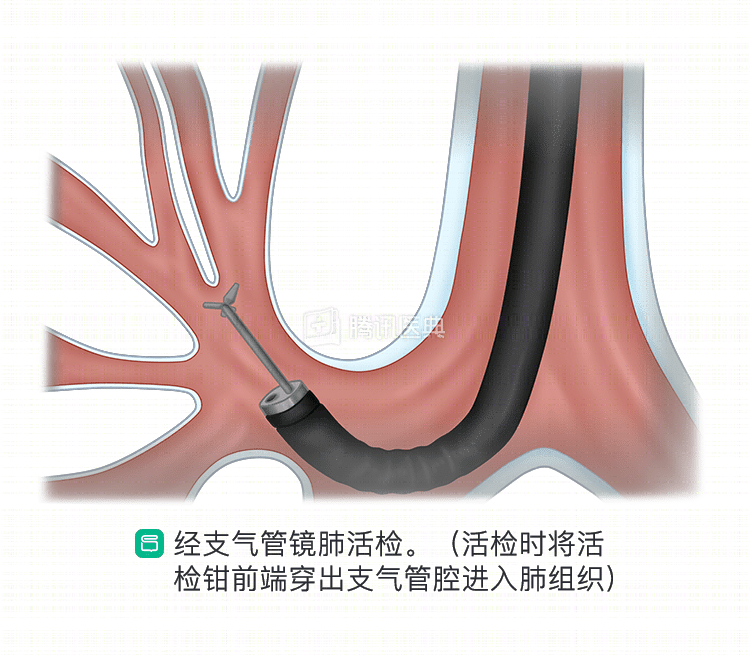
II. Percutaneous lung aspiration biopsy
If the tumor lesion is located in the peripheral lung, the physician may use a CT-guided percutaneous lung biopsy technique. Under CT guidance, a puncture needle is inserted into the tumor tissue and a sample is excised. Ultrasound-guided lung puncture biopsy may also be performed if the lesion is located immediately below the pleura.
The most common complications of percutaneous lung puncture are pneumothorax and hemoptysis, which are more likely to occur when the tumor tissue is richly vascularized. Before the test, the doctor will recommend a coagulation and platelet count test. Be sure to inform your doctor if you are taking anticoagulants, antiplatelet drugs, or have a history of coagulation disorders.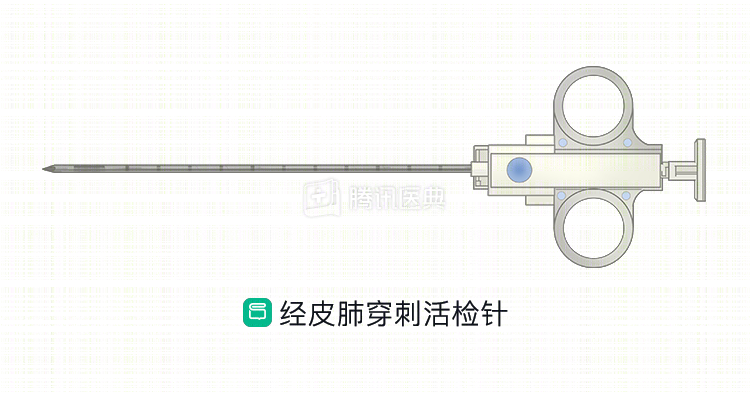
III. Biopsy of metastatic masses on the surface of the body
If lung cancer metastasizes to the surface of the body, body surface masses will be formed, especially supraclavicular and cervical lymph nodes, axillary and abdominal wall nodes. These superficial masses are easy to remove with less risk of bleeding, and doctors often choose to remove the masses intact for pathological examination to guide diagnosis and treatment.
IV. EBUS-guided lymph node aspiration and mediastinoscopic biopsy
If lung cancer has metastasized to the peribronchial lymph nodes, the physician will obtain tissue by needle aspiration of the lymph nodes under EBUS guidance. Sometimes mediastinoscopic biopsy of the lymph nodes may be indicated if the diagnosis is difficult to confirm with EBUS or to obtain more tumor tissue to facilitate the diagnosis. However, for tumors far from the bronchi and mediastinum, these two methods are less effective.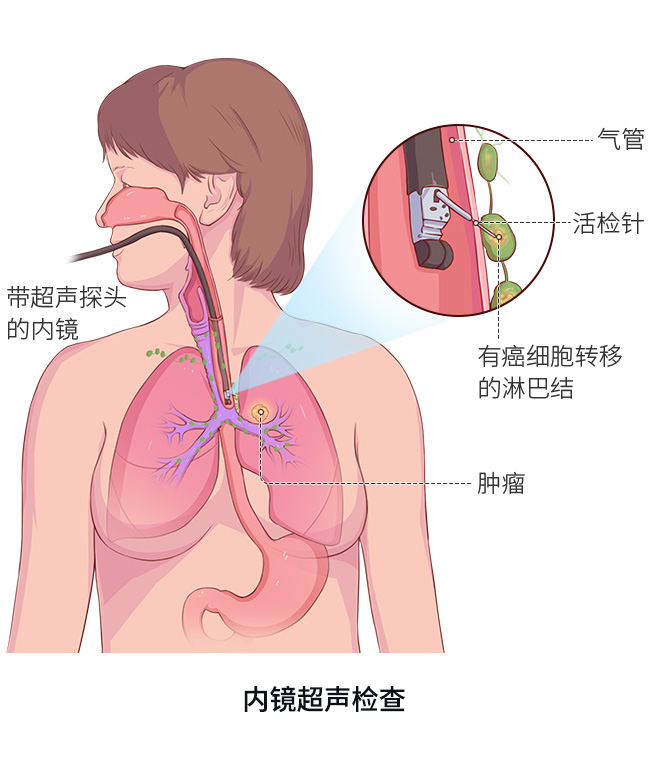
V. Internal thoracoscopy, pleural fluid and bronchoalveolar lavage fluid cytology
Clinically, if lung cancer tissue cannot be obtained by the above examinations, or if the risk is high, doctors will also use some additional methods to take samples: if lung cancer has metastasized to the pleura, direct biopsy of pleural tissue can be performed by thoracoscopy; if there is pleural effusion, pleural fluid can be extracted to collect the cancer cells inside.
At present, lung cancer treatment has entered the era of precision treatment, and many treatment plans and drugs are selected based on the results of lung cancer histology and molecular testing together. Obtaining sufficient and high quality samples is a prerequisite for accurate histological and molecular diagnosis.
Although physicians have a variety of “tools” to obtain tumor tissue and lung cancer pathology diagnosis rates are gradually increasing, there are still some special circumstances that make biopsy difficult or too risky to perform. In such complicated cases, doctors from radiotherapy, surgery, internal medicine, interventional medicine, and even pathology will consult and discuss how to make the diagnosis together.
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Wang Zhen, Deputy Chief Physician Dr. Kai Yin