Doctors sometimes mention that “according to current international (national) guidelines, we should ……..”. . What are “guidelines”? Why should doctors “follow” the guidelines?
Guidelines are usually written by experts from professional medical groups and are updated regularly as new research evidence becomes available. The guidelines are a summary of the “best current research evidence and expert experience”. The current mainstream guidelines are the NCCN guidelines in the United States and the CSCO guidelines in China.
So what do the guidelines say about the treatment of stage II non-small cell lung cancer?
NCCN guidelines
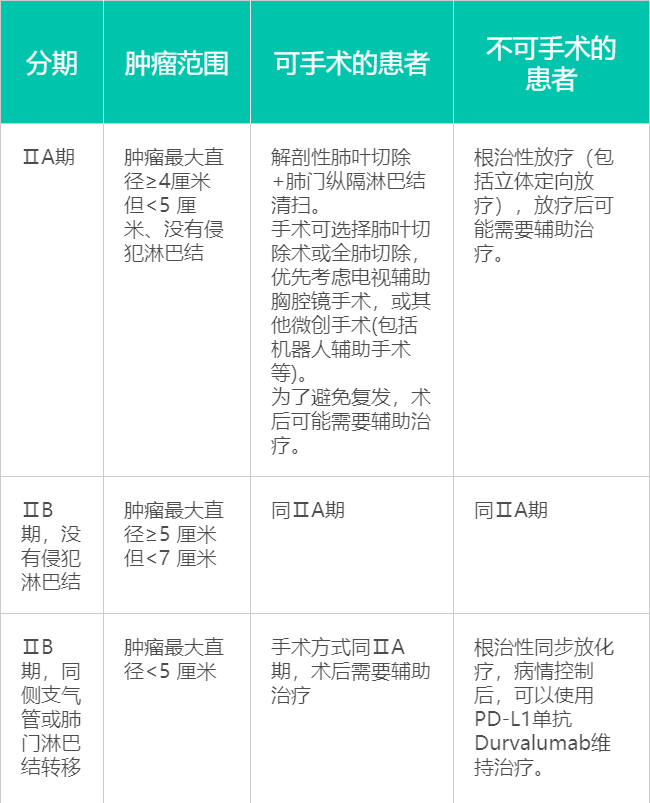
The “jargon” in the professional guidelines above is a little difficult to understand, so I’ll “translate” it for you. Stage II can be divided into two stages: stage IIA tumors are less than 5 cm and do not invade the surrounding lymph nodes; stage IIB tumors are between 5 and 7 cm, and in some patients the tumor invades the lymph nodes on the same side of the lesion.
Operable
In either case, surgery is the optimal option, as long as the body can tolerate it, to remove the diseased lobe or side of the lung while clearing the hilar mediastinal lymph nodes and clarifying the tumor stage. In the past, this was a major operation, requiring “open heart” surgery.
Nowadays, many hospitals can perform “minimally invasive” surgery thoracoscopically or with the help of a “robot”. The procedure can be done by making a few small holes in the chest wall and inserting instruments into the chest cavity.
Stage IIB (T3N0) patients with stage IIA and no lymph node metastases can be followed up or receive adjuvant platinum-containing double-drug therapy after surgery. In contrast, postoperative adjuvant therapy is recommended for stage IIB patients with lymph node metastases, usually by adjuvant chemotherapy. It is worth mentioning that clinical studies have confirmed that postoperative adjuvant targeted therapy in patients with stage IIA-IIIA EGFR gene mutations can benefit patients and may be included in clinical guidelines in the future.
Non-operable
If a patient is not a candidate for surgery because of poor lung function or the presence of other disease, the surgeon has two other weapons.
- Radiotherapy: If the tumor does not invade the lymph nodes, radiotherapy can be done, including “stereotactic radiotherapy,” which is a new technique that focuses the cancer more precisely and delivers a higher single dose, like an invisible “radiation knife. This is like an invisible “radiation knife”. After radiation therapy, your doctor may recommend adjuvant therapy to reduce the risk of recurrence.
- Synchronous radiotherapy: If there are lymph node metastases, your doctor may recommend “synchronized radiotherapy,” which means chemotherapy and radiotherapy are given simultaneously. It makes full use of the advantages of both therapies to achieve a “1+1>2” effect. After treatment, Durvalumab, a new immunotherapy drug, is recommended for further consolidation.
CSCO guidelines
As you can see, our guidelines are roughly the same as the US. If the patient is physically able to tolerate it, the surgeon’s first choice is to surgically remove the diseased lobe, and the surrounding lymph nodes need to be cleared. In stage IIB patients, postoperative chemotherapy is required.
Patients who are not candidates for surgery will be treated with radiation therapy. The radiotherapy is three-dimensional conformal radiotherapy. This type of radiotherapy is able to release radiation on the tumor tissue from several different angles to fit the shape of the tumor for optimal treatment. To avoid recurrence, radiation therapy can be followed by chemotherapy or directly by simultaneous radiation and chemotherapy.