
Osteoporosis is a “silent” disease that may not manifest itself in the early stages, and some people do not realize they have osteoporosis until they have pain that affects their lives, or even a fracture. Therefore, prevention of osteoporosis is an important topic for breast cancer patients.
As breast cancer treatment becomes more effective and patient survival continues to increase, tumor-related bone complications are becoming more common.
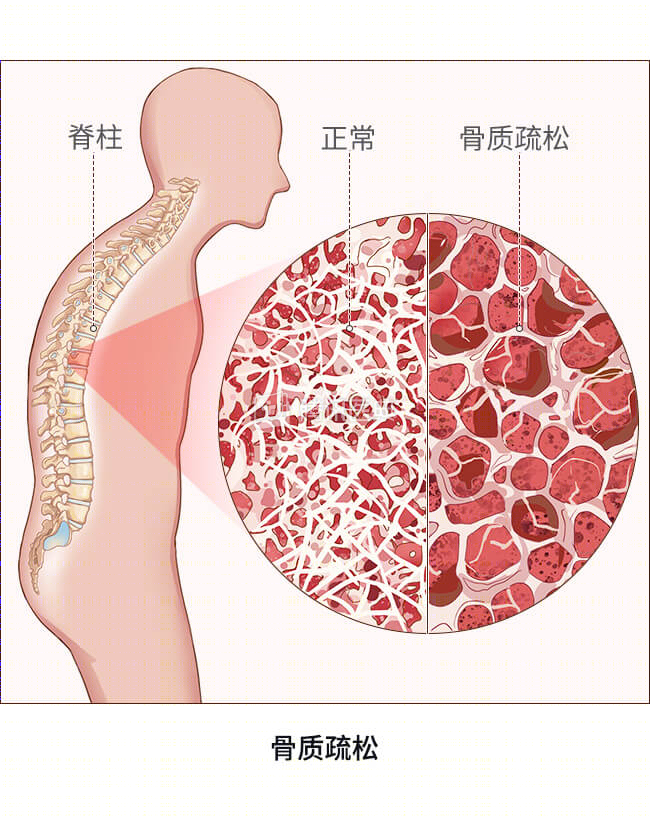
Bones are in a constant state of change throughout a person’s life, and typically, the body reaches a peak in bone mass around age 30 and then gradually decreases. Osteoporosis, a metabolic disease in which bone mass per unit volume decreases, is one of the common diseases in older adults, and the incidence of osteoporosis is higher in breast cancer patients.
Risk factors for osteoporosis
There are many risk factors for osteoporosis, the main ones include:
- Age over 60 years;
- A chronic low-calcium diet;
- Having a family history of osteoporosis;
- A bad lifestyle habit such as alcoholism, smoking, and long-term coffee and strong tea consumption;
- Wasting;
- Postmenopausal women or ovarian insufficiency and thus estrogen decline, etc.
Surgery, chemotherapy, radiotherapy, and endocrine therapy are all essential treatments for breast cancer patients, and the development of osteoporosis after comprehensive breast cancer treatment is the result of a combination of factors.
Chemotherapy and osteoporosis
For breast cancer patients undergoing chemotherapy, the causes of osteoporosis include:
- Chemotherapy drugs can disrupt the dynamic balance of bone formation and bone resorption, leading to bone loss and decreased bone density;
- Drugs used to control the side effects of chemotherapy, such as steroid hormones like dexamethasone, can lead to bone loss;
- Chemotherapy-induced gastrointestinal reactions can affect patients’ absorption of calcium, phosphorus, magnesium, and protein;
- Chemotherapy-induced hepatic and renal toxicity can affect vitamin D activity, which can cause bone loss;
- Premenopausal women receiving chemotherapy experience suppression of ovarian function and decreased estrogen levels, which can lead to decreased bone mass.
Endocrine therapy and osteoporosis
Estrogen and progesterone receptor-positive breast cancer patients account for about 60% or more of the total number of patients in China. Patients with hormone-dependent breast cancer all require endocrine therapy, and commonly used drugs include tamoxifen, toremifene, aromatase inhibitors (letrozole, anastrozole, exemestane), and so on. Endocrine therapy aims to reduce tumor recurrence by blocking estrogen receptors with drugs that inhibit estrogen synthesis and lower estrogen levels,
- The preferred endocrine treatment option for postmenopausal patients is an aromatase inhibitor, which directly blocks estrogen synthesis and reduces the body’s own production of estrogen levels. But at the same time, the bone is deprived of estrogen regulation, the activity of osteoblasts (cells that can turn into bone tissue) is reduced, and the activity of osteoclasts (cells that can break down bone tissue) is increased, further accelerating the process of osteoporosis in postmenopausal women and increasing the risk of fracture dramatically.
- A subset of premenopausal breast cancer patients will also choose pharmacologic ovarian function inhibitors (goserelin, leuprolide, etc.) to bring the body to a postmenopausal state, and the dramatic reduction in estrogen will also exacerbate bone loss.
Endocrine therapy is a long-term process, with the standard length of treatment being 5 years, and even longer for up to 10 years for patients with certain high-risk factors. Therefore, breast cancer patients on endocrine therapy should pay more attention to bone health to avoid excessive bone loss.
