Have you ever heard of treatments that “burn” or “freeze” tumor cells to death? How effective are they? This article will take a look at them.
Tumor ablation and cryotherapy
The treatment of “scalding” tumor cells to death is called “ablation” in professional circles; “freezing” is called “cryotherapy” in professional circles. The professional community is called “cryotherapy”.
The basic principle is similar. Under the guidance of CT or MRI, a probe or needle is inserted into the tumor, and the heat generated by electric current or ultra-low temperature generated by freezing agent (such as argon) is used to directly cause irreversible damage or coagulation of tumor cells in the focal tissue. The tumor cells in the focal tissue are irreversibly damaged or necrotic, and the surrounding tissues are coagulated, so that the tumor loses its blood supply and “dies”, which can also reduce the tumor metastasis.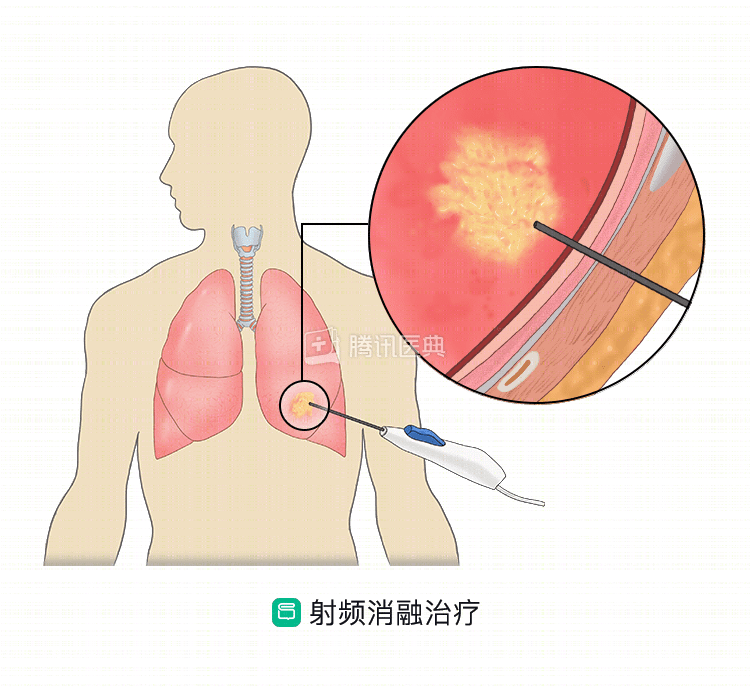
In addition, there are two other conditions in which open-chest or televised thoracoscopic-assisted ablation may be performed.
① lung tumors adjacent to important structures such as large blood vessels, lung hilum or heart.
② The lung tumor is found to be unresectable after open chest.
After freezing or ablation, the destroyed tumor tissue remains in the body and can also stimulate the body’s immunity to attack the tumor.
Which lung cancer patients might be considered?
Ablation and freezing are only appropriate for a small number of specific lung cancer patients.
Doctors may consider ablation/frozen techniques for early-stage, peripheral lung cancer if the patient cannot tolerate or is unwilling to undergo radical surgery or radiation therapy; or if there is a single recurrent isolated lesion after other treatments; a single lung (absence of one lung for various reasons); and multiple primary lung cancers with ≤3 tumors in both lungs. The conditions that need to be met are: the lesions should ideally be smaller than 3 cm and there are no metastases from other sites. In this case, ablation/freezing has the potential to achieve radical cure.
If multiple metastatic nodules in the lung have developed and are not curable, ablation/cryo has a place: that is, it is used to treat metastatic lesions that are still growing, on top of the main lesion being controlled. In this case, no more than 5 metastases in all lungs and no more than 3 in one lung with no other site of metastasis are required. The maximum diameter of multiple metastases is ≤ 3 cm and the maximum diameter of unilateral solitary metastases is ≤ 5 cm.
In addition, to relieve symptoms caused by localized lesions in some patients, sometimes physicians may consider using ablation/freezing to relieve pain.
It is important to note that ablation and freezing are not conventional treatments for lung cancer, but only local therapies that are “powerless” against widespread metastases throughout the body and should be used with caution on a case-by-case basis. The diagnosis of lung cancer needs to be confirmed before treatment, and it is best to undergo PET-CT to determine whether there are metastases elsewhere, as well as the location and size of the metastases before making a decision.
What are the possible adverse effects? How can I work with my doctor to deal with them?
.
Because this is an invasive treatment, patients with severe bleeding tendencies, relatively large pleural effusions on the treatment side, and poor overall health (PS score ≥3) are not candidates for this treatment.
In addition, the following conditions are not suitable for this therapy: infectious and radiological inflammation around the lesion that is not well controlled, skin infection and breakdown at the puncture site; severe pulmonary fibrosis, especially drug-induced pulmonary fibrosis; severe hepatic, renal, cardiac, pulmonary and cerebral insufficiency; severe anemia, dehydration and severe disturbances in nutritional metabolism that cannot be corrected or improved in a short period of time; severe systemic infection, high fever (> 38.5°C); and implantation of a pacemaker.
Overall, this is a relatively safe treatment. Adverse effects include: pain, pneumothorax, pleural reaction, bleeding, infection, etc., which need to be closely monitored and appropriate interventions applied when necessary.
In addition, some patients may suffer from “ablation syndrome”. This is due to the destruction of the tumor by the operation, and the necrotic tumor tissue is absorbed by the body, causing inflammatory reaction, mainly manifested as nausea, vomiting, low fever, weakness, etc., which usually lasts for 3~5 days, and some patients can last for 2 weeks. Doctors usually use non-steroidal drugs for anti-inflammation, more serious ones may be given small doses of glucocorticoids, while strengthening nutrition, most patients can tolerate it.
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Haiyan Tu, Deputy Chief Physician Dr. Yue-Li Sun Dr. Xiaoxiao Peng