
Stage 0 breast cancer (i.e., breast cancer in situ) is breast cancer that is relatively confined and has not yet broken through the basement membrane beneath the epithelial cells of the breast, also called non-invasive breast cancer. In the past, in situ breast cancer included intraductal carcinoma in situ and lobular carcinoma in situ. Because the characteristics of lobular carcinoma in situ are similar to those of benign breast disease in all aspects, lobular carcinoma in situ has been removed from breast carcinoma in situ and included in benign breast disease in the latest breast cancer staging. The only carcinoma in situ in the breast now includes only ductal carcinoma in situ (DCIS) in the breast.
Because breast carcinoma in situ does not break through the basement membrane, it does not spread and metastasize to surrounding tissues and usually has a better outcome. The goal of treatment for carcinoma in situ is to prevent the development of invasive breast cancer, and the treatment process is usually as follows.
Surgery
Breast-conserving surgery
Breast-conserving surgery may be considered if the requirements for breast-conserving surgery are met. Breast-conserving surgery removes only the tumor and some of the tissue surrounding the tumor, and is usually followed by radiation therapy.
Mastectomy
Currently, modified radical mastectomy is usually performed to remove the affected breast and some axillary lymph nodes, preserving the pectoral muscle.
Axillary lymph node management
For breast carcinoma in situ, a possible axillary lymph node management is an anterior sentinel lymph node biopsy, which is the first lymph nodes that must pass through for the primary tumor to develop lymph node metastasis. The advantage of this approach is that only a small number of lymph nodes in the sentinel lymph node are removed and the procedure is less invasive.
If breast-conserving surgery is performed, the surgeon typically does not perform a biopsy of the sentinel lymph nodes. If a mastectomy is performed, an anterior lymph node biopsy is usually performed at the time of surgery.
Breast reconstruction surgery
Doctors often discuss breast reconstruction if you undergo a total mastectomy. The main types of surgery in terms of timing are immediate breast reconstruction and delayed breast reconstruction, which is performed at the same time as a total mastectomy or months or years after the surgery.
Post-operative treatment
Postoperative local radiation therapy
Postoperative radiotherapy is generally not given to those who undergo mastectomy, but may be given if pathologic examination of the surgical specimen reveals a positive extensive cut margin.
After breast-conserving surgery, physicians typically recommend adjuvant postoperative whole-breast radiotherapy to destroy any local cancer cells that may remain and to reduce the recurrence rate. For patients with low-risk breast carcinoma in situ with very small lesions, the surgeon may not give postoperative radiotherapy if the negative surgical margins are wide.
Postoperative systemic adjuvant therapy
Since breast carcinoma in situ has a better outcome, the risks, such as side effects, of chemotherapy and targeted therapy may outweigh the benefits, so physicians generally do not give chemotherapy and targeted therapy.
Endocrine therapy has fewer side effects, and in estrogen receptor (ER) and/or progesterone receptor (PR) positive breast carcinoma in situ, adjuvant endocrine therapy may be given postoperatively to destroy any cancer cells that may remain and are not detected by current technology to reduce recurrence and also to prevent breast cancer in the contralateral breast.
- For ER- and/or PR-positive breast cancers in situ that have undergone breast-conserving surgery or unilateral mastectomy, physicians typically give endocrine therapy.
- For ER- and/or PR-positive mammary carcinoma in situ with bilateral mastectomy, the risk of postoperative breast cancer is low, and the decision may be made by the doctor taking into account the risk of recurrence, endocrine drug side effects, and the patient’s wishes.
- For ER- and PR-negative breast cancers, physicians generally do not give postoperative endocrine therapy because endocrine therapy does not prevent tumor recurrence.
When endocrine therapy is given, doctors individualize the decision to treat with tamoxifen or anastrozole, for example, based on the side effects of each drug, the patient’s menopausal status, and the patient’s wishes.
Follow-up visits
The purpose of follow-up is to detect and treat recurrent breast cancer and second primary breast cancer early and to evaluate treatment-related complications. Follow-up visits are usually every 6 to 12 months with a physical examination for the first 5 years after surgery, depending on the situation, and annually thereafter. Mammograms are typically performed every 6 to 12 months after breast-conserving surgery and every 12 months after mastectomy.
To have a good outcome, you should also maintain a healthy lifestyle, including appropriate exercise, a healthy diet, limiting alcohol consumption, and maintaining an ideal weight.
The specific course of treatment for breast cancer is influenced by factors such as disease, systemic status, risks of treatment, and the experience of the doctor, and the actual treatment requires the advice and recommendations of the doctor.
Summary
- In situ carcinoma of the breast has a better outcome, and the goal of treatment is to prevent the development of invasive breast cancer.
- Doctors usually use multimodal treatment, which may include surgery, radiation therapy, and endocrine therapy (for those who are estrogen and progesterone receptor positive).
- Surgical treatment is the basic treatment, with the remaining treatments as adjuvant therapy.
- After surgery, follow-up as required, adherence to treatment, and maintaining a healthy lifestyle are conducive to a good outcome.
Stage 0 breast cancer (carcinoma in situ) treatment flow chart
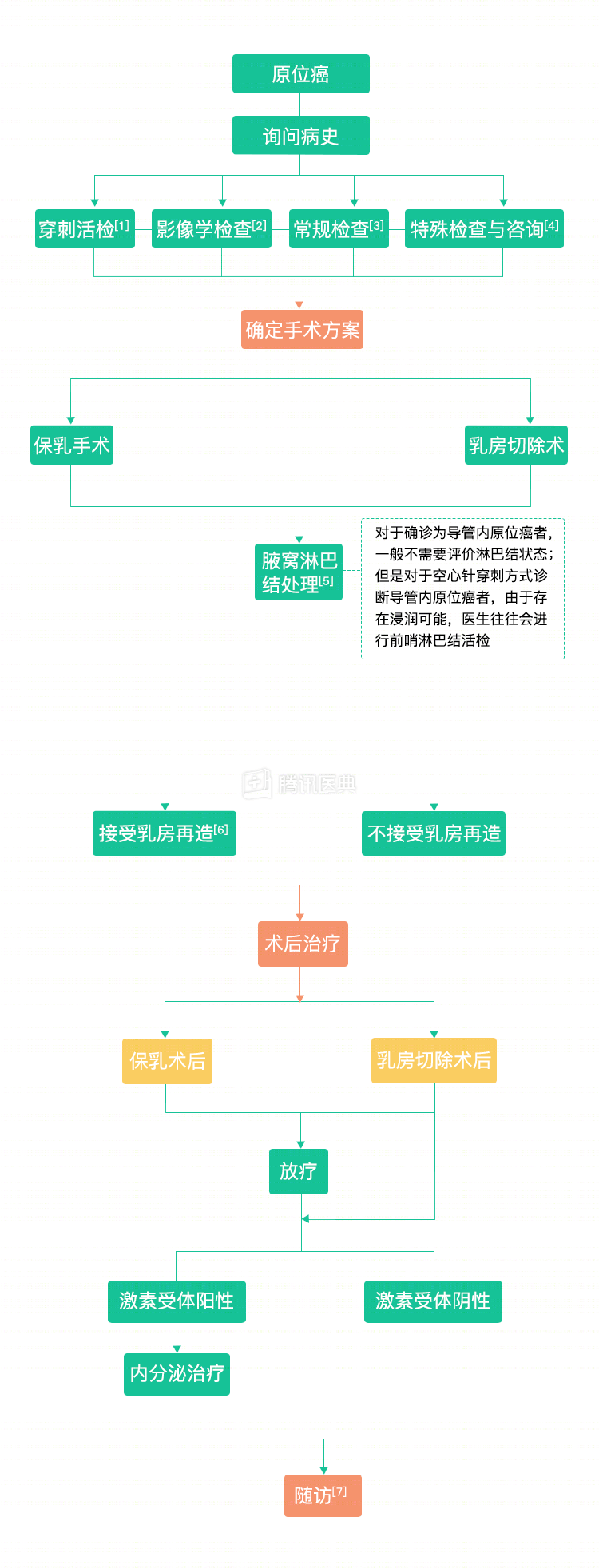
Notes:
- Puncture biopsy: The purpose of the biopsy is to obtain a tumor tissue specimen and perform biomarker testing for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER-2) to assist in the development of a treatment plan.
- Imaging: chest and abdominal imaging (X-ray, ultrasound, CT, MRI, etc.), bone scan (optional PET-CT may also be performed).
- Routine examination: physical examination, routine blood count, blood biochemistry.
- Special tests and consultations: genetic counseling, fertility counseling.
- Axillary lymph node management: Breast cancer surgery also includes removal and examination of the axillary lymph nodes to further confirm breast cancer staging and to determine if the cancer has spread outside the breast.
- Breast reconstruction: The procedure can be divided in terms of timing into primarily immediate breast reconstruction and deferred breast reconstruction, which is performed at the same time as total mastectomy or several months or years after surgery.
- Follow-up: Depending on the situation, follow-up may be 1 to 4 times per year for the first 5 years after surgery, with reviews every 3 months in years 1 to 2 and every 6 months in years 3 to 5. Mammography and other imaging, general physical examination, gynecologic examination, and bone density examination may be performed at follow-up visits.