Early-stage esophageal cancer can sometimes be cured by a “surgery without incisions” called endoscopic treatment. It is similar to gastroscopy in that the diseased tissue can be removed or inactivated directly in the body without opening the chest or abdomen. The efficacy is similar to that of surgery, with the added advantage of less trauma, faster recovery, and a survival rate of more than 95%.
Minimally invasive endoscopic treatments can be divided into two categories: endoscopic resection (ER) and non-endoscopic resection.
Endoscopic resection
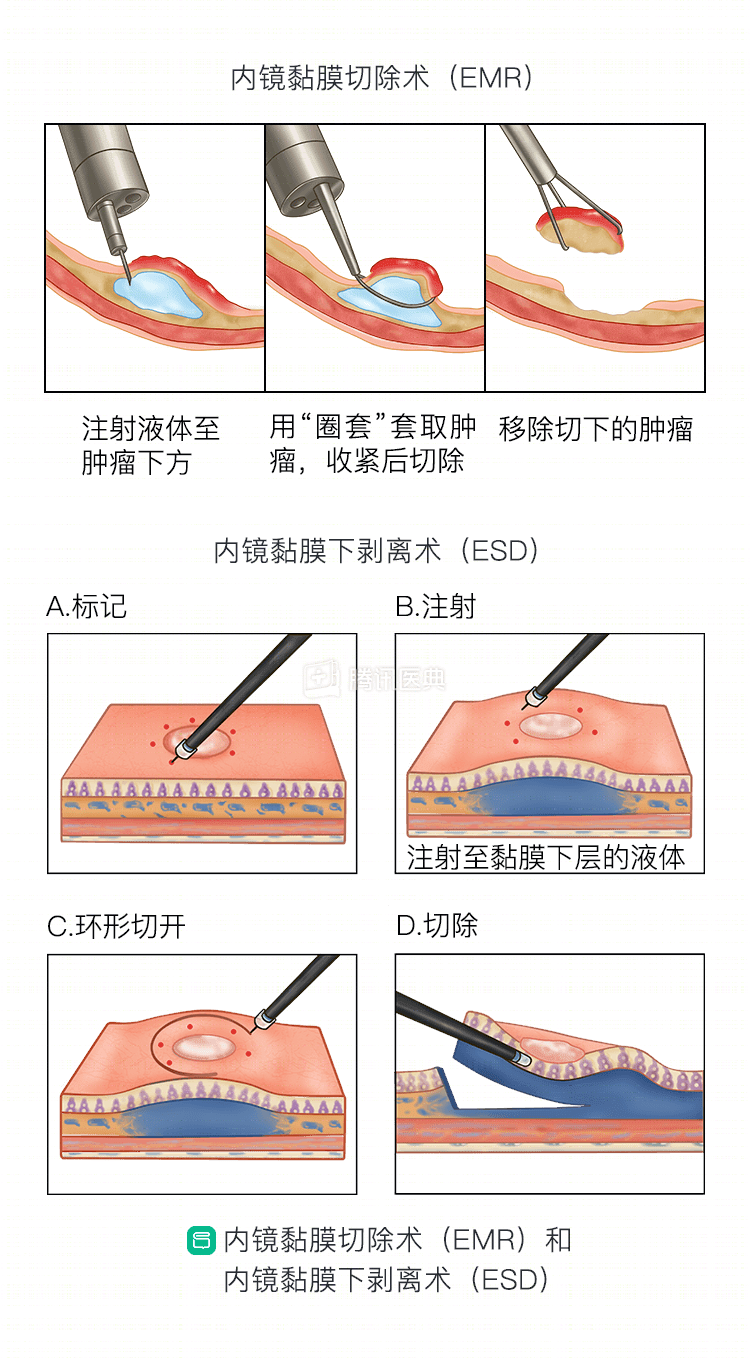
Including endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), and multiband mucosectomy (MBM).
Endoscopic submucosal dissection
In the 1990s, EMR was born. It removes a localized bulge of mucosa through an endoscopic electric knife. Smaller diameter (less than 2 cm) lesions can be removed in one complete pass; larger diameter lesions require multiple fractional resections (below).
It has the disadvantage that only mucosal lesions can be resected, and submucosal tumors cannot be completely removed; although it can perform segmental resection of large lesions, there is a high risk of local recurrence after surgery; it also cannot remove lesion tissue for pathologic biopsy and cannot provide a final diagnosis of tumor benignity or malignancy and staging.
Endoscopic submucosal dissection
ESD was reported in 2000 for early-stage esophageal cancer, which not only allows resection of lesions of any size and shape, but also treats them with the same results as surgery. In China, ESD began to be used in clinical practice in 2006.
It is like “eradicating” a tumor from the esophageal wall (pictured below). The surgeon lifts the mucosal layer with the endoscopic tool, and then peels off all of the mucosal layer and most of the submucosal tissue along the water cushion below the mucosal layer with an endoscopic electric knife.
In general, ESD is appropriate for mucosal lesions larger than 2 cm. Lesions smaller than 2 cm, although also available, have more complications and are riskier than EMR.
Multi-loop ligature mucosal resection
The surgeon attaches a special “snare” to the head of the gastroscope and then draws the lesion into a clear cap, releasing the snare ring and creating a “false polyp”. Next, the physician then applies the “snare” to the underside of the lesion, electrically removes it, and then removes the specimen and the snare ring. This can be done several times to completely remove the lesion .
MBM has been reported to be safer and more effective than EMR, with a lower incidence of postoperative complications than ESD. it has the advantage of separating the submucosal and muscular layers of the diseased tissue using the ligatures, avoiding complications such as perforation.
After resection of the lesion, the surgeon will treat the wound with endoscopic argon plasma coagulation (APC), hemostatic forceps, and titanium clips to eliminate residual lesions and exposed vessels to prevent delayed bleeding and perforation. after ESD and MBM treatment, the surgeon will also remove a portion of the cancer tissue and send it to pathology for pathological diagnosis.
To learn more about endoscopic resection and whether you are a candidate, read the following articles:
Endoscopic non-excisional treatment
Endoscopic non-excisional treatments include radiofrequency ablation (RFA), photodynamic therapy (PDT), argon plasma coagulation (APC), laser therapy, thermal probe therapy, and cryotherapy, etc. These techniques can be used either alone or in combination with endoscopic resection.
Endoscopic non-excisional therapy has unique advantages for some specific conditions of lesions, such as:
- Radiofrequency ablation
For multiple, long lesions or lesions involving the entire perimeter of the esophagus, with a low incidence of perforation and postoperative stricture.
- Cryotherapy
It can be used in patients who are not candidates for surgery and for whom endoscopic treatment is not effective. Its primary role is symptom relief rather than primary treatment.
- Photodynamic therapy
It can be used to manage large, early, multifocal lesions, and adverse effects such as photoallergic reactions, perforation, and stenosis should be noted after treatment.
However, non-excisional treatment cannot obtain tissue specimens for pathological examination to clarify whether the tumor is eradicated; therefore, close follow-up is required after treatment, and long-term efficacy needs to be further explored.
To learn more about endoscopic non-excisional therapy and whether you are a candidate, read the following article:
Two endoscopic treatment methods, how do I choose?
If you meet the indications for endoscopic treatment, then both types of approaches are capable of achieving radical cure. However, as mentioned earlier, non-excisional treatment does not allow for a definitive pathologic diagnosis. Therefore, if you are physically able to tolerate invasive treatment, the first choice, and the one recommended by your doctor, is endoscopic resection.
Co-written by:
Dr. Wang Police, Endoscopy Center, Peking University Cancer Hospital