Approved on.
Date of revision.
Posaconazole Enteric Dissolve Tablets Instructions
Please read the instruction manual carefully and use under the guidance of your physician
[Drug Name].
Generic Name: Posaconazole Enteric Tablets
Trade name: Noxafil® (Noxafil®)
English Name: Posaconazole Enteric-coated Tablets
Hanyu Pinyin: Boshakangzuo Changrongpian
[Ingredients
The main ingredient of this product: Posaconazole.
Chemical name of this product: 4-[4-[4-[4-[[(3R,5R)-5-(2,4-difluorophenyl)tetrahydro-5-(1H-1,2,4-triazole-1-methyl)-3-furan]methoxy]phenyl]-1-piperazinyl]phenyl]-2-[(1S,2S)-1-ethyl-2-hydroxypropyl]-2,4-dihydro-3H-1, 2,4-triazol-3-one
Chemical structure formula:
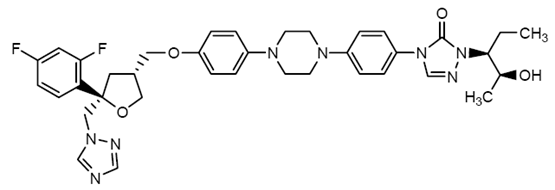

Molecular Formula: C37H42F2N8O4
Molecular weight: 700.8
Excipients: hydroxypropyl methyl cellulose acetate succinate, microcrystalline cellulose, hydroxypropyl cellulose, silicon dioxide, cross-linked sodium carboxymethylcellulose, magnesium stearate, ObadiahIIyellow (with polyvinyl alcohol, polyethylene glycol3350, titanium dioxide, talc, iron oxide yellow). family:Times New Roman”>
[Properties]This product is a film-coated tablet with one side inscribed with “100” inscribed on one side, appearing off-white after removing the coating.
[Indications
Prevention of invasive Aspergillus and Candida infections
This product is indicated for the prevention of13years and 13years and years and years and years. family:Arial”>year-old patients at increased risk of invasive Aspergillus and Candida infections due to severe immunodeficiency. These patients include those who underwent hematopoietic stem cell transplantation (HSCT) and then developed graft-versus-host disease (GVHD) or patients with hematologic malignancies in which chemotherapy results in prolonged neutropenia.
[Specification]100mg
[Dosage].
1. Dosage and Administration of Posaconazole Enteric Tablets
Dosage.
Table 1: Dosage of posaconazole enteric-coated tablets
|
Indications |
Dose and duration of treatment |
|
Prevention of invasive Aspergillus and Candida infections |
Load dose: 300mg (3 tablets of 100mg enteric-coated tablets) twice daily on day 1. Maintenance dose: 300 mg (100 mg enteric-coated 3 tablets) once daily starting on day 2. The duration of therapy depends on the degree of recovery from neutropenia or immunosuppression. |
2. Important Usage Notes for Posaconazole Enteric Tablets
-
Because the doses of posaconazole enteric-coated tablets and oral suspension are different, the two dosage forms should not be used interchangeably. The specific dosage instructions for Posaconazole Enteric Tablets and Posaconazole Oral Suspension should be followed for prescribing.
-
Posaconazole Enteric Solution should be swallowed whole and not broken, crushed, or chewed and then taken.
-
Posaconazole Enteric Tablets may be taken with or without food. Co-administration with food may increase oral absorption of posaconazole and optimize blood levels.
-
Posaconazole Enteric Tablets should be used for prophylactic dosing indications only. For the use of posaconazole in the treatment of oropharyngeal candidiasis, see the instructions for Posaconazole Oral Suspension.
-
Posaconazole Enteric Tablets provide a higher plasma drug exposure dose than posaconazole Oral Suspension under fasted and fed conditions and are the preferred oral dosage form for prophylactic indications.
-
Persons with severe diarrhea or vomiting should be closely monitored for breakthrough fungal infections when taking posaconazole enteric-coated tablets.
3. Dose adjustment in patients with renal insufficiency
Renal insufficiency does not have a significant effect on the pharmacokinetics of posaconazole. Therefore, no dose adjustment is required in patients with mild to severe renal impairment.
After a single dose of 400 mg oral suspension, mild (eGFR: 50- 80 ml/min/1.73 m2, n = 6) or moderate (eGFR: 20-49 ml/min/1.73 m2, n = 6) renal insufficiency does not have a significant effect on the pharmacokinetics of posaconazole and therefore no dose adjustment is required in patients with mild to moderate renal insufficiency. In patients with severe renal insufficiency (eGFR: < 20 ml/min/1.73 m2), mean plasma exposure levels (AUC) were similar to those in patients with normal renal function (eGFR: > 80 ml/min/1.73 m2); however, compared with other renal insufficiency groups (coefficient of variation < ; 40%), there was higher variability in the range of AUC estimates in patients with severe renal insufficiency (coefficient of variation= 96%). Because of the variability in exposure levels, close monitoring of breakthrough fungal infections in patients with severe renal impairment is necessary. The above dose-adjustment recommendations also apply to posaconazole enteric-coated tablets, but posaconazole enteric-coated tablets have not been studied specifically.
4. Dose adjustment for patients with hepatic insufficiency.
In patients with mild (Child-Pugh class A, N = 6), moderate (Child-Pugh class B, N = 6), or severe (Child-Pugh class C, N = 6) hepatic insufficiency, a single oral dose of posaconazole oral suspension 400 mg After a single oral dose of posaconazole oral suspension 400 mg, the mean AUC was elevated by 43%, 27% and 21%, respectively, compared to subjects with normal liver function (N = 18). Mean Cmax was increased by 1%, increased by 40%, and decreased by 34% in patients with mild, moderate, or severe hepatic insufficiency, respectively, compared with subjects with normal liver function. Mean apparent oral clearance (CL/F) was decreased by 18%, 36% and 28% in patients with mild, moderate and severe hepatic insufficiency, respectively, compared to subjects with normal liver function. Elimination half-lives (t1/2) were 27 hours, 39 hours, 27 hours, and 43 hours in subjects with normal liver function and in patients with mild, moderate, or severe hepatic insufficiency, respectively.
In patients with mild to severe hepatic insufficiency (Child-Pugh class A, B, or C), no dose adjustment is recommended for this product. The above dose-adjustment recommendations also apply to posaconazole enteric-coated tablets, but posaconazole enteric-coated tablets have not been studied specifically.
5. Gender
The pharmacokinetics of posaconazole are similar in men and women. No dose adjustment of this product based on gender is required.
6. Ethnicity
The pharmacokinetic properties of posaconazole are not significantly affected by ethnicity. Dose adjustment of this product based on ethnicity is not required.
7. Weight
Posaconazole pharmacokinetic models suggest that patients weighing >120 kg may have lower posaconazole exposure doses, and therefore close monitoring for breakthrough fungal infections is recommended in patients weighing >120 kg.
[Adverse effects
- Serious adverse reactions and other important adverse reactions
The following serious adverse reactions and other important adverse reactions are discussed in detail elsewhere in this instruction manual:
- Allergic reactions.
- arrhythmias andQTinterval prolongation.
- Hepatotoxicity.
2,
Clinical trial experience
Because clinical trials are conducted under a variety of conditions, the incidence of adverse reactions in clinical trials of this product cannot be directly compared to the incidence in clinical trials of other drugs and is not representative of the actual incidence in clinical practice. The types of adverse reactions reported in clinical trials with posaconazole enteric-coated tablets are generally similar to those reported in clinical trials with posaconazole oral suspension.
Posaconazole enteric-coated tablets clinical trial experience
The safety of posaconazole enteric-coated tablets has been investigated in230patients enrolled in the clinical study. Patients were enrolled for prophylactic antifungal administration (enteric-coated tablet study1) concurrently with posaconazole enteric-coated tablets for noncomparative pharmacokinetic and safety trials. Patients with underlying lesions of compromised immune system including hematologic malignancies, neutropenia after chemotherapy, hematopoietic stem cell transplantation (HSCT) followed by graft-versus-host disease (GVHD). The total patient population62%was male with a mean age of 51years old (range19-78years),17% ≥65years,< span style="font-family:Times New Roman">93% were Caucasian, 16% were of Hispanic origin. The median duration of treatment with posaconazole was 28days, and the median duration of treatment with posaconazole was 28days,20patients received 200 mg daily< span style="font-family:Arial">dose, 210patients receiving dailydose. span>300mgdaily (the firstdose in each group) New Roman”>1day were administered twice). Table2 indicates the daily dose in the posaconazole enteric-coated tablet study. family:Times New Roman”>300 mgtreated patients observed an incidence≥10%of treatment-related adverse reactions.
Table 2: Number (%) of treatment-related adverse reactions reported in subjects treated with posaconazole enteric-coated tablets Study 1: 300 mg daily dose: incidence at least 10%
|
Body System Preferred terminology |
Posaconazole Enteric Tablets (300mg) (n=210) |
||
|
subjects who reported any adverse reactions |
201 |
(99) |
|
|
Diseases of the blood and lymphatic system |
|||
|
< span style="color:black; font-size:10pt">Anemia |
22 |
(10) |
|
|
thrombocytopenia |
29 |
(14) |
|
|
Gastrointestinal Disorders |
|||
|
Abdominal pain |
23 |
(11) > |
|
|
Constipation |
20 |
||
|
Diarrhea |
61 |
< p style="text-align: center">(29) | |
|
Nasty |
56 |
(27) |
|
|
Vomiting |
28 |
(13) |
|
|
Systemic disease and dosing site conditions |
|||
|
Lackluster |
20 |
(10) |
|
|
Chills |
22 |
(10) > |
|
|
Mucosal inflammation < |
29 |
||
|
33 |
< p style="text-align: center">(16) | ||
|
Fever |
59 |
(28) |
|
|
Metabolic and nutritional disorders |
|||
|
Hypokalemia |
46 |
< span style="color:black; font-size:10pt">(22) |
|
|
Low magnesiumemia |
20 |
(10) |
|
|
Neurological Disorders |
|||
|
Headache |
30 |
(14) |
|
|
Respiratory, thoracic, and mediastinal disorders |
|||
|
Cough |
35 |
(17) |
|
|
Rhinorrhea |
30 |
(14) > |
|
|
Skin and Subcutaneous tissue disorders |
|||
|
Rash |
34 |
(16) > |
|
|
Vascular Disease |
|||
|
hypertension |
23 > |
(11) |
|
The most frequently reported (>25%) adverse reactions to treatment with posaconazole enteric-coated tablets 300 mg once daily were diarrhea, fever, and nausea.
The most common adverse reaction leading to discontinuation of posaconazole enteric-coated tablets 300 mg once daily treatment was nausea (2%).
Posaconazole Oral Suspension Clinical Trial Safety Experience
In1844the safety of posaconazole oral suspension treatment was evaluated in patients. These included 605 patients enrolled in the active-controlled prophylaxis study, patients enrolled in the active-controlled oropharyngeal candidiasis study< span style="font-family:Times New Roman">557patients, 239patients, and 443< span style="font-family:Arial">patients. These patients represented a diverse population, including patients with impaired immune function such as malignant hematologic disease, neutropenia after chemotherapy, graft-versus-host reaction after hematopoietic stem cell transplantation, andHIVinfected patients, and non-neutropenic patients. This patient population was 71%male with a mean age of 42 years old (range8to84years,6% of patients≥ 65years,1%of patients< 18years),and64% were white,16% and family:Arial”>are Hispanic,36%are non-white (including14% of blacks). 171 patients received≥ 6months of posaconazole treatment, of whom58patients received≥ 12months of posaconazole treatment. Table3shows the posaconazole prevention study with an incidence greater than10% of the adverse reactions that occurred during treatment. Table4shows oropharyngeal candidiasis ( OPC)/refractory oropharyngeal candidiasis (rOPC) study with an incidence of at least10% of adverse reactions on treatment.
Prevention of Aspergillus and Candida:
In2in randomized, comparative prevention studies (oral suspension studies1and< span style="font-family:Times New Roman">2), in severely immunocompromised patients, posaconazole oral suspension200 mg(daily3sessions) versus fluconazole400 mg(daily) regimen. span>1time) or Itraconazole200 mg200 mg(2times daily) or Itraconazole2 times) scenarios were compared for safety.
Prevention of the most frequently reported adverse reactions in clinical studies (> 30%) included fever, diarrhea, and nausea.
Adverse reactions in prevention clinical studies that most often led to discontinuation of posaconazole therapy were associated with gastrointestinal conditions, specifically nausea ( 2%), vomiting (2%) and elevated liver enzymes (2%).
Table 3: Posaconazole Oral Suspension Study 1 and Study 2
Number of randomized subjects reporting adverse reactions on treatment (%).
Frequency of occurrence of at least 10% in the posaconazole oral suspension or fluconazole treatment group (pooled preventive safety analysis)
|
Posaconazole |
Fluconazole |
Itraconazole < /td> | |
|
Subjects who reported any adverse reactions |
595 (98) |
531(99) |
58 (100) |
|
Systemic -Whole Body Disease |
|||
|
Fever Headache |
274 (45) 171 (28) |
254 (47) 141 (26) |
32 (55) 23 (40) |
|
Chills and shivers Fatigue Oedema of the legs |
122 (20) 101 (17) 93 (15) |
87 (16) 98 (18) 67(12) |
17 (29) 5 (9) 11 (19) |
|
Anorexia Dizziness |
92 (15) 64(11) |
94(17) |
16 (28) 5 (9) |
|
Oedema Weakness |
< span style="font-size:10pt">54(9) 51(8) |
68(13) |
< span style="font-size:10pt">8(14) 2 (3) |
| < p>General cardiovascular disease | |||
|
hypertension Low blood pressure |
< span style="font-size:10pt">106 (18) 83 (14) |
88 (16) 79 (15) |
3(5) 10 (17) |
|
Diseases of the blood and lymphatic system |
|||
|
Anemia Neutropenia |
149 (25) 141 (23) |
124 (23) 122 (23) |
16 (28) 23 (40) |
|
Reproductive and breast disorders |
|||
|
Vaginal bleeding* |
24(10) |
20(9) |
3(12) |
|
Gastrointestinal System Disorders< |
|||
|
Diarrhea Nausea Vomiting Abdominal pain Constipation Indigestion |
< span style="font-size:10pt">256 (42) < span style="font-size:10pt">232 (38) 174 (29) 161 (27) 126 (21) 61 (10) |
212 (39) 198 (37) 173 (32) 147 (27) 94 (17) 50 (9) |
35 (60) 30 (52) 24 (41) 21 (36) 10 (17) 6 (10) |
|
Heart rate and rhythm disorders |
|||
|
Tachycardia |
72(12) |
75(14) |
3(5) |
|
Infectious Diseases |
|||
|
Pharyngitis |
=”padding-left: 3px; padding-right: 3px; border-top: none; border-left: none; border-bottom: solid 0.5pt; border-right: solid 0.5pt”>
71(12) |
< span style="font-size:10pt">60(11) |
12(21)< /span> |
|
Diseases of the liver and biliary system |
Bilirubinemia |
59(10) |
51(9) |
11(19) |
|
Hypokalemia Hypomagnesemia Hyperglycemia Hypocalcemia |
< span style="font-size:10pt">181 (30) < span style="font-size:10pt">110 (18) 68 (11) 56(9) |
142 (26) 84 (16) 76 (14) 55 (10) |
30 (52) 11 (19) 2 (3) 5 (9) |
| < p>Musculoskeletal disorders | |||
|
Musculoskeletal pain Joint pain Back pain |
< span style="font-size:10pt">95 (16) < span style="font-size:10pt">69 (11) 63 (10) |
82 (15) 67 (12) 66(12) |
9(16) 5 (9) 4 (7) |
| < p>Platelets, bleeding and coagulation disorders | |||
|
Thrombocytopenia Stasis |
< span style="font-size:10pt">175 (29) 64 (11) |
146 (27) 54 (10) |
20 (34) 9 (16) |
|
Mental illness |
|||
|
Insomnia |
103(17) |
92(17) |
11(19) |
|
Respiratory Disease |
|||
|
Cough Hard to breathe Epistaxis |
< span style="font-size:10pt">146 (24) < span style="font-size:10pt">121 (20) 82 (14) |
130 (24) 116 (22) 73 (14) |
14 (24) 15 (26) |
|
Dermal and subcutaneous tissue disorders |
|||
|
< span style="font-size:10pt">Rash Itching |
< span style="font-size:10pt">113 (19) 69 (11) |
96 (18) 62 (12) |
25 (43) 11 (19) |
|
* Percentage of gender-specific adverse events calculated based on the number of male/female patients. |
|||
HIV-infected subjects with oropharyngeal candidiasis.
In 2 randomized, controlled studies of oropharyngeal candidiasis, the safety of 557 HIV-infected patients receiving posaconazole oral suspension ≤400 mg once daily was compared with the safety of 262 HIV-infected patients receiving fluconazole 100 mg once daily was compared.
Also239patients who developed refractory oropharyngeal candidiasisHIVinfection In2items on refractory oropharyngeal candidiasis (rOPC) received posaconazole treatment in a noncomparative clinical trial. Of these subjects, 149 received daily800 mgdose and the remaining subjects received doses≤ 400 mg. span>, daily1treatment.
InOPC/rOPCstudies, the most common adverse reactions included fever, diarrhea, nausea, headache, vomiting, and cough.
In controlOPC The most frequent adverse reactions leading to discontinuation of posaconazole therapy in the pooled studies included respiratory insufficiency (1%) and pneumonia (1%). In refractoryOPCsummary studies, the most frequent adverse reactions leading to discontinuation of posaconazole therapy includedAIDS(7%) and respiratory insufficiency (3%).
Table 4: Adverse reactions occurring in treatment with a frequency of at least 10% in the Posaconazole Oral Suspension OPC study (treated population)
|
Body System Preferred terminology |
Number of subjects (%) |
||
|
Contrast OPC Summary |
< p style="text-align: center; background: white">Difficult to treat OPC Summary |
||
|
Posaconazole |
Fluconazole |
Posaconazole n = 239 |
|
|
Subjects reporting any adverse events* |
356(64) |
175(67) |
< span style="font-family:Times New Roman">221(92) |
|
Total Body – Total Body Disease |
|||
|
Fever Headache Anorexia Fatigue Weakness Chills Pain |
34(66) 44(8)) =”font-family:Times New Roman”> 10(2)) =”font-family:Times New Roman”> 18(3)) =”font-family:Times New Roman”> 9(2)) =”font-family:Times New Roman”> 2(< 1) 4(1) > |
22(8)) 23(9)) =”font-family:Times New Roman”> 4(2)) =”font-family:Times New Roman”> 12(5)) =”font-family:Times New Roman”> 5(2)) =”font-family:Times New Roman”> 4(2)) =”font-family:Times New Roman”> 2(1) > |
82(34)) 47(20) 46(19) 31(13) 31(13) 29(12) 27(11) |
|
Diseases of the blood and lymphatic system |
|||
|
Neutropenia Anemia |
21(44) 11(2) > |
8(3) 5(2) > |
39(16)) 34(14) |
|
Gastrointestinal System Disorders |
|||
|
Diarrhea Nausea Vomiting Abdominal pain |
58(1010) 48(9)) =”font-family:Times New Roman”> 37(7)) =”font-family:Times New Roman”> 27(5) > |
34(13)) 30(11) 18(7) =”font-family:Times New Roman”> 17(6) > |
70(29)) 70(29) 67(28) 43(18) |
|
Infectious Diseases |
|||
|
Oral candidiasis Herpes simplex Pneumonia |
3(1) 16(3)) =”font-family:Times New Roman”> 17(3) > |
1(< 1) 8(3)) =”font-family:Times New Roman”> 6(2) > |
28(12)) 26(11) 25(10) |
|
Metabolic and nutritional diseases |
|||
|
Weight loss Dehydration |
4(1) 4(1) > |
2(1) 7(3) > |
33(14)) 27(11) |
|
Mental illness |
|||
|
Insomnia |
8 >(1) |
3 (1) |
|
|
< span style="font-size:10pt">Respiratory Disease |
|||
|
Cough Difficulty breathing |
18(3) 8(1) > |
11(4)) 8(3) > |
60(25)) 28(12) |
|
Dermal and subcutaneous tissue disorders |
|||
|
Rash Increased sweating |
15(3) 13(2) > |
10(4)) 5(2) > |
36(15)) 23(10) |
|
OPC = oropharyngeal candidiasis. *Number of subjects reporting at least 1 treatment-emergent adverse event during the study period, regardless of the relationship to treatment. Subjects may report more than 1 adverse event. |
|||
Adverse reactions are more common in the summary of patients with refractory oropharyngeal candidiasis. In these highly immunodeficient patients with combined advancedHIVinfection, serious adverse reactions (SARs) occurred at a rate of55< /span>% (132/239 ). The most common serious adverse reactions were fever (13%) and neutropenia ( “font-family:Times New Roman”>10%).
Less common adverse reactions: in posaconazole prophylaxis,OPC/rOPCor other clinically meaningful patient incidence reported during clinical trials <5% of adverse reactions include:
- style=”margin-left: 36pt”>
-
Hematologic and lymphatic system: hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, and exacerbation of neutropenia.
-
Endocrine system: Adrenal insufficiency.
-
Neurological: sensory abnormalities.
-
Immune System: Allergic reactions. (See [Contraindications])
-
Heart: tip-twisting ventricular tachycardia. (See [Caution])
-
Vascular: Pulmonary embolism.
-
Gastrointestinal: Pancreatitis
-
Hepatobiliary System: Bilirubinemia, elevated liver enzyme levels, abnormal liver function, hepatitis hepatomegaly, jaundice, elevated ASTlevels, ALTlevels are elevated.
-
Metabolism and Nutrition: Hypokalemia.
-
Platelets, bleeding and coagulation: Thrombocytopenia.
-
Renal and urinary system: Acute renal failure.
Clinical laboratory test values.
In healthy volunteers and patients, elevated values of liver function test parameters were not associated with elevated posaconazole plasma concentrations.
The number of patients in the prevention study whose liver function test results changed from a universal toxicity criteria (CTC) of 0, 1, or 2 degrees at baseline to 3 or 4 degrees during the study period can be seen in Table 5.
Table 5: Posaconazole Oral Suspension Study 1 and Study 2, Change in Liver Function Test Results from CTC 0, 1, or 2 Degrees to 3 or 4 Degrees at Baseline
|
Number of patients with change (%)* |
|||
|
< span style="font-size:10pt">Posaconazole Oral Suspension Study 1 |
|||
|
Lab parameters |
Posaconazole (n = 301) |
Fluconazole (n = 299) |
|
|
Aspartate Aminotransferase (AST) |
11/266(4) |
13/266(5) |
|
|
Alanine aminotransferase ( ALT) |
47/271(17) |
39/272(14) |
|
|
< span style="font-size:10pt">Bilirubin |
24/271(9) |
20/275(7) |
|
|
Alkaline phosphatase |
9/271(3) |
8/271(3) | |
|
Posaconazole Oral Suspension Study 2 |
|||
|
Posaconazole (n = 304) |
Fluconazole/Itraconazole (n = 298) |
||
|
Aspartate Aminotransferase (AST) |
9/286(3) |
5/280(2) |
|
|
Alanine Aminotransferase (ALT)< |
18/289(6) |
13/284(5) |
|
|
Bilirubin |
20/290(7) |
||
|
Alkaline phosphatase |
4/281( 1) |
1/276 (<1) |
|
|
*Changes from 0 to 2 degrees in the baseline period to 3 or 4 degrees during the study period. These data are expressed in the form of X/Y, where X indicates the number of patients meeting the criteria shown and Y indicates the number of patients with a baseline period observation and at least 1 post-baseline observation. CTC = common toxicity criteria; AST = aspartate aminotransferase; ALT = alanine aminotransferase. |
|||
The number of patients with oropharyngeal candidiasis who developed clinically significant liver function test (LFT) abnormalities at any time during the study period can be found in Table 6 (some patients had liver function test abnormalities prior to initiation of study drug therapy abnormalities).
Table 6: Posaconazole Oral Suspension Study: Clinically Significant Laboratory Test Abnormalities, Disregarding Baseline Values
|
Lab Tests |
Contrast |
Difficult to treat |
|
|
Posaconazole |
Fluconazole |
Posaconazole |
|
|
n = 557 (%) |
n = 262 (%) |
n = 239 (%) |
|
|
ALT > 3.0x upper limit of normal |
16/537(3) |
13/254(5) |
25/226(11) |
|
AST > 3.0 |
33/537(6) |
26/254(10) |
39/223(17) |
|
Total bilirubin > 1.5x upper limit of normal |
15/536(3) |
5/254(2) |
9/197(5) |
|
Alkaline phosphatase > 3.0x upper limit of normal |
17/535(3) |
15/253(6) |
24/190 (13) |
|
< span style="font-size:10pt">ALT = alanine aminotransferase; AST = aspartate aminotransferase. |
|||
3. Post-marketing experience
No clinically meaningful adverse reactions that were not disclosed during clinical trials have been identified since the launch of this product.
[Contraindication
-
Allergic reactions
This product is contraindicated in patients with hypersensitivity to posaconazole, any component of this product, or other azole antifungals.
-
In combination with sirolimus
The combination of this product with sirolimus is prohibited. Co-administration of this product with sirolimus can result in an approximately 9fold increase in sirolimus blood levels, which can lead to sirolimus toxicity.
-
withCYP3A4substrate combination can lead toQTprolonged interval
Prohibit the use of this product withCYP3A4substrates, as the combination can lead toQT interval is prolonged. Co-administration of this product withCYP3A4substrates pimozide and quinidine can lead to increased plasma concentrations of these drugs, resulting inprolonged QTcinterval and tip-twist ventricular tachycardia.
- Primarily throughCYP3A4metabolized byHMG-CoAreductase inhibitors span>
Prohibits the combination of this product with a reductase inhibitor primarily via CYP3A4. “font-family:Arial”>metabolizedHMG-CoAreductase inhibitors, such as ator vincristine, lovastatin, and simvastatin. Because of the increased blood levels of these drugs in combination, they can lead to rhabdomyolysis.
-
Co-administration with ergot alkaloids
Posaconazole causes elevated plasma concentrations of ergot alkaloids (ergotamine and dihydroergotamine), which may lead to ergot toxicity.
[Precautions].
1,< /span>
Drug interactions with neurocalciferol inhibitors
Coadministration of this product with cyclosporine or tacrolimus may result in elevated trough values of whole blood concentrations of these neurocalcine inhibitors. Nephrotoxicity and cerebral leukoaraiosis (including fatal cases) have been reported in patients with elevated concentrations of cyclosporine or tacrolimus in clinical efficacy studies. The trough values of cyclosporine or tacrolimus should be monitored frequently during and after discontinuation of posaconazole therapy and the dose of cyclosporine or tacrolimus should be adjusted accordingly.
2,. span>
arrhythmias andQT Interval extension
Some azoles, including posaconazole, cause ECGprolonged QTinterval. In addition, cases of tip-twist ventricular tachycardia have been reported in patients on posaconazole.
Multiple time-matched ECG analysis in healthy volunteers showedthe mean QTcinterval without any elevation. Receipt of posaconazole oral suspension400 mg per day was recorded at baseline and steady state style=”font-family:Times New Roman”>2times per day, accompanied by a high-fat diet of 173 healthy male and female volunteers (aged 18- 85years) in multiple time-matched ECGs collected within 12hours. In this pooled analysis, after dosing at the recommended clinical dose,QTcinterval (Fridericia) mean change from baseline of -5 msec. It was also found in a small number of subjects given placebo (n = 16) ) family:Times New Roman”>QTc(F) interval reduction (-3 msec). Placebo-adjusted maximumQTc(F) interval mean change relative to baseline< 0 msec (-8 msec). Healthy subjects receiving posaconazole did not developQTc(F)interval≥ 500 msecorQTc(F) interval is elevated compared to baseline≥ 60 msec.
Posaconazole should be used with caution in patients at risk for pharmacologic arrhythmic conditions. This product should not be used with drugs known to prolong the QTcinterval and to be part of the CYP3A4substrates in combination. Blood potassium, magnesium, and calcium should be corrected as much as possible before starting posaconazole therapy.
This product must be used with caution in patients who have experienced arrhythmic conditions, such as:
-
Congenital or acquiredQTcprolonged interval
-
Cardiomyopathy, especially heart failure
-
Sinus bradycardia
-
Symptomatic arrhythmia has developed
-
The combination is known to causedrugs with a prolonged QTcinterval (except those mentioned in contraindications).
Electrolyte disturbances, particularly potassium, magnesium, or calcium levels, should be monitored and corrected as necessary before and during posaconazole therapy.
Posaconazole isCYP3A4< span style="font-family:Arial">inhibitor, and during treatment with other drugs that are metabolized through CYP3A4 metabolized during drug therapy and only under special circumstances (see Drug Interactions).
3,
HepatotoxicityHepatic adverse reactions (e.g., mild to moderate elevations in alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, total bilirubin levels and/or clinical hepatitis) have occurred in clinical trials. Elevated liver function test parameters are usually reversible upon discontinuation of therapy, and in some cases, the results of these tests may return to normal when drug therapy is not suspended. Patients with severe underlying disease (e.g., hematologic malignancies) have experienced more severe hepatic adverse reactions during posaconazole therapy, including cholestasis or liver failure, and even death. These severe hepatic adverse reactions were seen primarily in subjects treated with posaconazole oral solution 800 mg daily (400 mg twice daily or 200 mg four times daily) in a clinical trial.
Liver function tests must be evaluated at the start of posaconazole treatment and during treatment. Patients who develop abnormal liver function tests with posaconazole therapy must be monitored for the development of more severe liver injury. Patient management must include laboratory assessment of liver function (especially liver function tests and bilirubin). Posaconazole therapy must be discontinued if clinical signs and symptoms are consistent with liver disease progression and may be associated with posaconazole.
4, renal insufficiency
Because of the variability in posaconazole enteric-coated tablets and oral suspension exposure, breakthrough fungal infections in patients with severe renal insufficiency must be closely monitored.
5, in combination with midazolam , in combination with midazolam
Coadministration of this product with midazolam results in an approximately 5-fold increase in midazolam plasma concentrations. In turn, elevated midazolam plasma concentrations enhance and prolong the hypnotic and sedative effects. Treated patients must be monitored closely for adverse reactions due to high midazolam plasma concentrations, and benzodiazepine receptor antagonists must be available to reverse these reactions.
6, Vincristine toxicity
Neurotoxicity and other serious adverse reactions associated with the combination of vincristine and azole antifungals, including posaconazole, include seizures, peripheral neuropathy, inappropriate antidiuretic hormone secretion syndrome, and paralytic intestinal obstruction. Treatment with azole antifungals, including posaconazole, may be reserved for patients using perphenazine, including vincristine, when no other antimicrobial therapy is available.
7, others<
Allergic reactions
There is no information regarding cross-sensitivity of posaconazole with other azole antifungals. The allergy should be monitored when posaconazole is administered to patients who are allergic to other azoles.
Gastrointestinal disorders
There are limited pharmacokinetic data regarding patients with severe gastrointestinal dysfunction (e.g., severe diarrhea). Close monitoring of breakthrough fungal infections is necessary in patients with severe diarrhea or vomiting.
Rifamycin antimicrobial agents (rifampin, rifabutin), specific anticonvulsants (phenytoin, carbamazepine, phenobarbital, paracetamol), and efavirenz< /span>
Posaconazole concentrations can decrease significantly during combination therapy;
Therefore, the combination of posaconazole must be avoided unless the benefits to the patient outweigh the risks.Impact on ability to drive and operate machines
Due to certain reported adverse effects of posaconazole (e.g., dizziness, drowsiness, etc.) that potentially could affect the ability to drive/operate machinery, this product should be used with caution if driving or operating machinery is required.
[For Pregnant and Lactating Women
Pregnancy
Adequate and well-controlled studies have not been conducted in pregnant women. This product should not be used in pregnant women unless the potential benefit outweighs the potential risk to the fetus.
In rats, posaconazole at doses ≥ 27 mg/kg (≥ 1.4 times the exposure level of 400 mg based on steady-state plasma concentrations in healthy volunteers with an oral suspension twice-daily dosing regimen) resulted in skeletal deformities (cranial deformities and rib deficiencies. In rats, the dose at which no skeletal deformities were observed (no-effect dose) was 9 mg/kg at an exposure level of 400 mg, 0.7 times the oral suspension twice-daily dosing regimen. In rabbits, no deformities were observed at the maximum dose of 80 mg/kg. In rabbits, the no-effect dose was 20 mg/kg, while higher doses of 40 mg/kg and 80 mg/kg resulted in increased fetal uptake, with these doses producing exposure levels 2.9 or 5.2 times higher than the 400 mg oral suspension twice-daily regimen, respectively. In rabbits, reduced body weight gain and reduced litter size were observed in females at the 80 mg/kg dose.
Lactating women
Posaconazole is excreted into the milk of lactating rats. It is not known whether this product is excreted into human milk. Because of the potential for serious adverse reactions in nursing infants, the decision to discontinue nursing or discontinue drug therapy should be made considering the importance of the drug to the mother.
Fertility
Posaconazole at a maximum dose of 180 mg/kg (exposure level of 300 mg, 3.4 times the twice-daily dosing regimen based on steady-state plasma concentrations in healthy volunteer subjects) or 45 mg/kg (exposure level of 300 mg, 2.6 times the twice-daily dosing regimen) did not have any effect on fertility in male or female rats, respectively. There were no effects on fertility in male or female rats, respectively. There is no clinical experience evaluating the effects of posaconazole on human fertility.
[Pediatric Dosage].
The safety and efficacy of posaconazole oral suspension and posaconazole enteric-coated tablets have been demonstrated in the 13- to 17-year-old age group. Adequate and well-controlled adult studies provide evidence for the use of posaconazole in these populations. The safety and efficacy of posaconazole in pediatric patients under 13 years of age (from birth to 12 years) have not been established.
A total of 12 patients aged 13 to 17 years received a dose of posaconazole oral suspension 600 mg daily (200 mg three times daily) for the prevention of invasive fungal infections. The safety profile in these patients younger than 18 years of age was similar to that of adults. Based on pharmacokinetic data in 10 pediatric patients, the mean steady-state posaconazole concentrations (Cavg) were similar in these patients and adults (≥ 18 years of age). In a study involving another indication, a total of 136 patients aged 11 months to less than 18 years were treated with posaconazole oral suspension at a total daily dose of up to 18 mg/kg, divided into three daily doses, and approximately 50% of patients (rather than a predetermined 90% of patients) achieved a target steady-state posaconazole concentration (Cavg) exposure between 500 ng/mL and less than between 2500ng/mL.
[Geriatric Dosing
Thirty-eight of 230 patients (17%) treated with posaconazole enteric coated tablets were >65 years of age. The pharmacokinetics of posaconazole enteric-coated tablets were similar in younger and older subjects. No overall differences in safety were observed between older and younger patients, and therefore no adjustment of dosing in older patients is recommended.
Of the 605 patients randomized to posaconazole oral suspension in the prophylactic clinical trial, 63 (10%) were ≥65 years of age. In addition, 48 patients treated with ≥800 mg daily posaconazole in another indication were ≥65 years of age. There was no overall difference in the safety of posaconazole between older and younger patients.
In younger and older (≥ 65< span style="font-family:Arial">years) subjects, the pharmacokinetics of posaconazole oral suspension were similar. In elderly patients, no age-based dose adjustment of this product is required.
There were no overall differences in pharmacokinetics and safety between older and younger subjects during clinical trials, but greater sensitivity in some older adults cannot be ruled out.
[Drug Interactions].
Posaconazole is primarily administered via UDP glucosylation for metabolism and is pglycoprotein (P-gp) substrate for pump-out action. Therefore, inhibitors or inducers of these clearance pathways can have an impact on posaconazole plasma concentrations. Unless the benefits to the patient outweigh the risks, posaconazole should generally be avoided with concomitant administration of drugs that may reduce posaconazole plasma concentrations. If such drugs must be administered, patients should be closely monitored for breakthrough fungal infections.
Posaconazole is alsoCYP3A4 a drug that can be used to treat fungal infections. /span>a potent inhibitor of CYP3A4. Thus posaconazole can increase plasma concentrations of drugs that are metabolized primarily by CYP3A4.
1, by < CYP3A4metabolized by immunosuppressants
Sirolimus: oral posaconazole administered in repeated doses in healthy subjects (daily2times oral suspension400 mgfor16days), sirolimus (2mgsingle dose) of CC sub>maxandAUCby an average of 6.7fold and 8.9fold. When starting posaconazole therapy in patients taking sirolimus, the dose of sirolimus should be reduced (e.g., to 1/10), and frequent monitoring of sirolimus whole blood trough concentrations. Sirolimus concentrations should be monitored prior to initiation of dosing, during concomitant dosing, and at the termination of posaconazole therapy, and sirolimus dose should be adjusted accordingly.
Tacrolimus: Posaconazole can cause tacrolimus (0.05 mg/kgsingle dose) of Cmax< span style="font-family:Arial">andAUCvalues were significantly increased, respectively span>121%and358%358%. Reduce the dose of tacrolimus to approximately one-third of the initial dose at the start of posaconazole therapy. The tacrolimus troughs should be monitored frequently during and after discontinuation of posaconazole therapy and the tacrolimus dose should be adjusted accordingly.
Cyclosporine: after starting posaconazole therapy, posaconazole oral suspension200 mgdaily1times can result in elevated cyclosporine whole blood concentrations in heart transplant patients. It is recommended that the dose of cyclosporine be reduced to approximately three-quarters of the initial dose at the time posaconazole therapy is initiated. The trough values of cyclosporine whole blood concentrations should be monitored frequently during and after discontinuation of posaconazole therapy, and cyclosporine dose should be adjusted accordingly.
2,. span>CYP3A4substrate
Posaconazole withCYP3A4substrates such as pimozide and quinidine in combination can lead to elevated plasma concentrations of the above drugs, resulting inQTc< span style="font-family:Arial">interval prolongation and tip-twisting ventricular tachycardia. Therefore, posaconazole is contraindicated in combination with these drugs.
3, by < /span>CYP3A4metabolized byHMG-CoAreductase inhibitors (statins)
Orally administered posaconazole in repeated doses (daily1time oral suspension50,100,200 mg, continuous13day) of simvastatin (40 mgsingle dose)< span style="font-family:Times New Roman">CmaxandAUC increased on average by 7.4 respectively family:Arial”>to11.4fold andfold respectively. family:Times New Roman”>5.7to10.6fold. Increased plasma concentrations of HMG-CoAreductase inhibitors may accompany rhabdomyolysis. Prohibition of posaconazole with CYP3A4metabolism primarily via family:Times New Roman”>HMG-CoAreductase inhibitors are taken concurrently.
4, ergot Alkaloids
.Most ergot alkaloids are CYP3A4substrates. Posaconazole causes elevated plasma concentrations of ergot alkaloids (ergotamine and dihydroergotamine), which may lead to ergot toxicity. Therefore, the combination of posaconazole and ergot alkaloids is prohibited.
5, by < CYP3A4metabolized by benzodiazepines
Posaconazole coadministered with midazolam results in elevated midazolam plasma concentrations of approximately5fold. Oral posaconazole repeated dose administration (2times daily oral suspension200 mg for7days) respectively, increasing intravenous administration of midazolam (0.4 mgsingle dose)CmaxandandAUCaverage1.3 times and4.6 times. 2times dailyPosaconazole Oral Suspension400 mg for7day, respectively, increasing midazolamCmaxandAUCof1.6 times and6.2fold. Posaconazole2doses were increased by oral midazolam (2mgorally as a single dose)Cmax andAUCof2.2fold and4.54.5times. In addition, concomitant oral posaconazole (200 mgor or400 mgorally administered suspension) can result in a change in the mean terminal half-life of midazolam from approximately3-4hours to8-10hours. In contrast, elevated plasma concentrations of midazolam enhance and prolong the hypnotic and sedative effects.
Posaconazole is associated with other drugs that are effective through CYP3A4metabolized benzodiazepines (e.g., alprazolam, triazolam) can lead to elevated plasma concentrations of these benzodiazepines when coadministered. Treated patients must be monitored closely for the occurrence of excessive plasma concentrations of benzodiazepines metabolized via CYP3A4. adverse reactions, and benzodiazepine receptor antagonists must be available to reverse these reactions. Dose adjustment of benzodiazepines metabolized by CYP3A4is recommended during concomitant administration with posaconazole.
6, anti, anti span>HIVdrugs
BecauseHIV< span style="font-family:Arial">protease inhibitors as CYP3A4substrates. Posaconazole is expected to increase the plasma levels of these antiretroviral agents. In healthy subjects, repeated dose administration of oral posaconazole (daily2times oral suspensions =”font-family:Times New Roman”>400 mgconsecutively7< span style="font-family:Arial">days) respectively with an average increase of atazanavir (daily1 times300 mg, continuously7days) ofCmax =”font-family:Arial”>andAUC2.6times and3.7fold. In healthy subjects, when taking ritonavir (daily1times300 mgazanavir plus100 mg< span style="font-family:Arial">ritonavir for 7days) as an adjunctive regimen When oral posaconazole is repeatedly administered (2times dailyoral suspensions400 mg continuously7days) respectively, a smaller average increase in atazanavirCmaxandAUC1.5times and2.5fold. Frequent monitoring for adverse events associated with antiretroviral agents (CYP3A4enzyme-acting agents) is recommended during concomitant administration with posaconazole and toxicity.
Efavirenz: Efavirenz induces UDP-glucocerebrosidase and significantly reduces posaconazole plasma concentrations. 400 mgdaily1times may reduce posaconazoleCmaxandAUCof45%and50%. Avoiding efavirenz in combination with posaconazole is recommended unless the benefit outweighs the risk.
Ritonavir and atazanavir: Ritonavir and atazanavir are administered viaCYP3A4metabolism, and posaconazole causes elevated plasma concentrations of these drugs . Adverse reactions and toxicity should be monitored frequently during coadministration with posaconazole, and dose adjustments should be made for ritonavir and atazanavir.
Fosamprenavir: Combining fosamprenavir and posaconazole may result in lower posaconazole plasma concentrations. Close monitoring of breakthrough fungal infections is recommended if concomitant administration is required. Fosamprenavir (700 mgdaily2times a day for10consecutive family:Arial”>day) repeated dosing reduced posaconazole (day1day oral suspension daily >1time200 mg and the next day oral suspension daily2times200 mg, followed by continuous8days of oral suspension daily2times400 mg)CmaxandAUCof21%and23%.
7, rifabutin Ting
Rifabutin inducesUDP-glucocerebrosidase, rifabutin300 mg1times dailyreduces posaconazoleCmaxandAUCAUCof43%and49%. Rifabutin is also metabolized via CYP3A4. Therefore, the coadministration of rifabutin with posaconazole leads to rifabutinCmaxand AUC were elevated by 31%and72%. The combination of posaconazole with rifabutin should be avoided unless the benefit to the patient outweighs the risk. However, if a combination is required, close monitoring for breakthrough fungal infections and frequent monitoring for complete blood counts and adverse effects (e.g., uveitis, leukopenia) is recommended due to elevated rifabutin plasma concentrations.
8, phenytoin
Phenytoin inducesUDP-glucosidase, phenytoin200 mg1times dailyreduces posaconazole respectively family:Times New Roman”>CmaxandAUCof41%andand span>50%. Phenytoin is also metabolized via CYP3A4. Therefore, coadministration of phenytoin with posaconazole results in elevated phenytoin plasma concentrations. The combination of posaconazole with phenytoin should be avoided unless the benefit to the patient outweighs the risk. However, if coadministration is required, close monitoring of breakthrough fungal infections, frequent monitoring of phenytoin concentrations, and consideration of phenytoin dose reduction are recommended when coadministered with posaconazole.
9, gastric acid inhibitors/neutralizers
No clinically relevant effects on posaconazole pharmacokinetics have been observed when posaconazole enteric-coated tablets are used concomitantly with antacids, H2 receptor antagonists, and proton pump inhibitors. Concomitant use of posaconazole enteric tablets with antacids, H2 receptor antagonists, and proton pump inhibitors does not require adjustment of posaconazole enteric tablets dosing.
10, perphenazine
Most periwinkle alkaloids (e.g. periwinkle and periwinkle) areCYP3A4substrates. Serious adverse reactions have been associated with the combination of vincristine and azole antifungals, including posaconazole (see “Precautions”). Posaconazole can cause elevated plasma concentrations of Vincristine, which can lead to neurotoxicity and other serious adverse reactions. Therefore, treatment with azole antifungals, including posaconazole, may be reserved for patients on vincristine, including vincristine, when no other antimicrobial treatment options are available.
11, by CYP3A4metabolized by calcium channel blockers
Posaconazole may lead to a significant increase in calcium metabolism via CYP3A4increased plasma concentrations of metabolized calcium channel blockers (e.g., verapamil, diltiazem, nifedipine, nicardipine, felodipine). Frequent monitoring for adverse reactions and toxicity associated with calcium channel blockers is recommended during combination therapy. Dose reduction of calcium channel blockers may be required.
12. Digoxin
Elevated digoxin plasma concentrations have been reported in patients receiving digoxin in combination with posaconazole. Therefore, monitoring of plasma concentrations of digoxin is recommended during combination therapy.
13, gastrointestinal Power drugs
Concurrent administration of metoclopramide with posaconazole enteric-coated tablets does not affect the pharmacokinetics of posaconazole. No adjustment of posaconazole enteric-coated tablets dosing is required when administered concomitantly with metoclopramide.
14, Glipizide Pyrazine
A single 10-mg dose of glipizide had no clinically significant effect on the Cmax and AUC of posaconazole. Although no dose adjustment of glipizide is required when posaconazole is coadministered with glipizide, monitoring of glucose concentrations is nevertheless recommended.
15. Zidovudine (AZT), lamivudine (3TC), and indinavir
Clinical studies have shown no clinically significant effects of zidovudine, lamivudine, or indinavir when taken concomitantly with posaconazole. Therefore, concomitant administration with these drugs does not require dose adjustment.
[Drug overdose].
There has been no experience with drug overdose with posaconazole enteric-coated tablets.
During the clinical trial, some patients were treated with the maximum dose of posaconazole oral suspension of 1600 mg daily, and these patients experienced adverse events that did not differ from the results observed at the lower dose. In addition, an unintentional overdose occurred in one patient who received 1200 mg twice daily for 3 days. The investigators found no drug-related adverse events.
Posaconazole was not cleared by hemodialysis.
[Clinical trial].
Posaconazole Enteric Dissolve Tablets Bridging Study Summary
Study 5615 was a noncomparative multicenter study designed to evaluate the pharmacokinetic profile, safety, and tolerability of posaconazole enteric-coated tablets. The study population was similar to that of patients previously enrolled in the pivotal posaconazole oral suspension. Pharmacokinetic data and safety data from Study 5615 were bridged to existing data from the oral suspension (including efficacy data).
The subject population for Study 5615 included 1) patients with AML or MDS who had recently received chemotherapy and had developed or were expected to develop severe neutropenia, or 2) patients who had received HSCT and were receiving immunosuppressive therapy for the prevention or treatment of GVHD. Two different dosing groups were evaluated in this study: 200 mg twice daily on day 1, followed by 200 mg once daily (part IA); and 300 mg twice daily on day 1, followed by 300 mg once daily (parts IB and 2).
For all subjects in part 1 and a subgroup of subjects in part 2, serial PK samples were collected on day 1 and on day 8 when steady state was reached. In addition, for a larger population of subjects, sparse PK samples were collected before the next dose administration (Cmin) on the days when steady state was reached. Based on the mean Cmin concentration, the predicted mean concentration (Cavg) can be calculated for 186 subjects given 300 mg of the drug. PK analysis of patients with Cavg showed that 81% of patients receiving 300 mg of the drug once daily achieved steady-state predicted Cavg (500 -2500 ng/mL). 1 subject (<1 %) developed pCavg below 500 ng/mL, and 19% developed pCavg above 500 ng/mL. Nineteen percent of subjects developed pCavg above 2500 ng/mL. The mean steady-state pCavg achieved by subjects was 1970 ng/mL.
In Table 7 are shown the results of comparative exposure levels (Cavg) after administration of posaconazole enteric tablets and posaconazole oral suspension at therapeutic doses in patients as described in the quartile analysis. Exposure levels after tablet administration were generally higher than those after posaconazole oral suspension administration, but there was overlap.
Table 7: Cavg Quartile Analysis of Posaconazole Enteric Tablets and Oral Suspensions in Pivotal Patient Studies
=”padding-left: 1px; padding-right: 1px; border-top: solid 0.5pt; border-left: none; border-bottom: solid 0.5pt; border-right: solid 0.5pt”>
Posaconazole Enteric Tablets
< td colspan="3" style="padding-left: 1px; padding-right: 1px; border-top: solid 0.5pt; border-left: none; border-right: solid 0.5pt">
Posaconazole Oral Suspension
< tr>
In AML and HSCT patients
Prevention Study 5615
In GVHD in patients with
Prevention Study 316
Prevention Study 316
In neutrophil reduction in patients with
Prevention Study 1899
Treatment-Invasive Aspergillosis
Study 0041
300mg once daily
(Day 1, 300 mg twice daily)*
200 mg three times daily
< strong>200 mg three times daily
200 mg four times daily (inpatient), followed by 400 mg twice daily
Quartiles
pCav range
(ng/mL)
Cav range
(ng/mL)
Cav range
(ng/mL)
Cav range
(ng/mL)
Q1
442 – 1223
442 – 1223 =”padding-left: 1px; padding-right: 1px; border-top: none; border-left: none; border-bottom: solid 0.5pt; border-right: solid 0.5pt”>
22 -557
90 – 322
55 -277
Q2
1240 – 1710
557 – 915
322 – 490
290 – 544
Q3
1719 -2291
915 – 1563
490 – 734
550 – 861
Q4
2304 – 9523
1563 – 3650
734 – 2200
877 -2010
< /td>
pCav: Forecast Cav
Cav = the average concentration measured at steady state
*20 patients receiving 200 mg of drug once daily (day 1 200 mg twice daily)
Trial 117 is a multicenter, 2-subgroup trial designed to evaluate the pharmacokinetic (PK) profile and safety of posaconazole enteric-coated tablets in Chinese subjects at high risk for invasive fungal infections (IFI), and to compare the safety profile with that of previous posaconazole enteric-coated tablets. A clinical trial designed to evaluate the pharmacokinetic (PK) profile and safety of posaconazole enteric tablets in Chinese subjects at high risk for invasive fungal infections (IFI) and to bridge the drug exposure and safety with those established in previous posaconazole oral suspension studies.
The study enrolled 65 Chinese subjects with neutropenia after chemotherapy for acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS). Subjects received posaconazole enteric-coated tablets 300 mg, administered twice daily on day 1 and then 300 mg once daily for a minimum of 8 days and a maximum of 28 days. The first 20 subjects enrolled were assigned to subgroup 1, and the next 45 subjects were assigned to subgroup 2. Subgroup 1 subjects underwent intensive PK sampling on day 1 and steady-state day 8, and all 65 subjects underwent several sparse PK samplings before the next dose to reach steady state.
Predicted Cavg (pCavg) was calculated for 64 evaluable subjects based on mean Cmin concentrations. All subjects had pCavg above 500 ng/ml; 59/64 (92.2%), 4/64 (6.3%) and 1/64 (1.6%) subjects had pCavg in the range of 500 – 2500 ng/mL, 2500 – 3750 ng/mL and > 3750 ng/mL ranges. The mean predicted Cavg when subjects reached steady state was 1770 ng/mL.
Summary of the Posaconazole Enteric Tablets China PK Study
Trial 111 was a randomized, open, single-dose, three-phase (A: 300 mg posaconazole enteric-coated tablets administered on an empty stomach; B: 300 mg posaconazole intravenous infusion solution administered on an empty stomach; C: 300 mg posaconazole enteric-coated tablets administered after a high-fat breakfast) crossover in 18 healthy Chinese adult male and female subjects. Design of the clinical trial. One of the main objectives was to evaluate the pharmacokinetic profile of posaconazole enteric-coated tablets administered as a single dose in the fasting state in healthy Chinese subjects. This study found that the PK exposure of posaconazole enteric-coated tablets administered in the fasting state was within the range of previous clinical studies. The Tmax of posaconazole enteric-coated tablets after administration in the fasted state was 4 h and the half-life was 25.21 h. The geometric mean values of AUC0-inf and Cmax were 25,263 hr*ng/mL and 674.5 ng/mL, respectively.
Posaconazole Oral Suspension Clinical Study Summary
1. Posaconazole oral suspension prevents Aspergillus and Candida infections
Two randomized, controlled studies of posaconazole for the prevention of invasive fungal infections (IFIs) in patients at increased risk due to severe immune system deficiency were conducted.
The first study (Oral Suspension Study 1) was a randomized, double-blind clinical trial comparing posaconazole oral suspension (200 mg 3 times daily) with fluconazole capsules (400 mg once daily) for the prevention of invasive fungal infections in allogeneic hematopoietic stem cell transplant (HSCT) recipients presenting with graft-versus-host disease (GVHD). Effectiveness of prophylaxis was assessed using a composite endpoint including proven/very suspicious invasive fungal infection, death, or use of systemic antifungal therapy (patients may meet more than 1 criterion). This trial evaluated all patients 7 days after the end of study treatment and 16 weeks after randomization to the group. The mean duration of treatment was similar between the 2 treatment groups (80 and 77 days in the posaconazole and fluconazole treatment groups, respectively). The results of the oral suspension study 1 are shown in Table 8.
Table 8: Results of blinded clinical study 1 on oral suspension for the prevention of invasive fungal infections in all patients undergoing randomized grouping for hematopoietic stem cell transplantation (HSCT) and graft-versus-host disease (GVHD)
Posaconazole
Fluconazole
n = 301
n = 299
After treatment7days
< span style="font-family:Arial">Clinical Failure*
50 (17%)
55 (18%)
Reason for failure:
confirmed/suspected invasive fungal infection =”font-family:Times New Roman”>
7 < (2%)
22 (7%) >
(Aspergillus)
3 (1%)
17(6< span style="font-family:Arial">%)
< span style="font-family:Arial; font-size:10pt">(Candida)
1 (< 1%)
3 (1%)
(Other)
3 (1%)
2 < span style="font-family:Arial">(1%)
All Dead
>
22(7%)
24(8%)
Before death After confirmed/suspected fungal infection
< p style="text-align: center; margin-left: 37pt">2(< 1%) 6 (2%)
SAF†
27< span style="font-family:Arial">(9%)
25< span style="font-family:Arial">(8%)
until week16week span>
clinical failure*‡
99(33%)
110(37%)
Reason for failure:
< /td> Confirmed/suspected invasive fungal infection
16< span style="font-family:Arial">(5%)
27 (9%)
(Aspergillus)
7(2%)
21(< span style="font-family:Times New Roman">7%)
(Candida)
4(1%)
4 (1%)
(Other)
5(2%)
2 (1%)
All Dead< span style="font-family:Times New Roman">
58(19%)
59(20) %)
< span style="font-size:10pt">Confirmed before death/suspected fungal infection
10(3%)
16(5%)
SAF†
26 (9%)
30(10%)
No incident missed visits§
24 (8%)
30 (10%)
* Patients may meet more than 1 failure definition criteria .
† Criteria for use of systemic antifungal therapy (SAF) as defined by the trial protocol (empirical/IFI use > 4 consecutive days).
‡ 95% confidence interval (posaconazole-fluconazole) = (-11.5%, +3.7%).
§ Patients who were lost to follow-up (not observed within 112 days) and did not meet another clinical failure endpoint. These patients were considered to have failed.
Study 2 (Oral Mix Study 2) is a study in neutropenic patients receiving cytotoxic chemotherapy for acute myeloid leukemia or myelodysplastic syndrome. A randomized, open study comparing posaconazole oral suspension (200 mg three times daily), fluconazole suspension (400 mg once daily), or itraconazole oral solution (200 mg twice daily) for the prevention of invasive fungal infections in patients with neutropenia receiving cytotoxic chemotherapy for acute myeloid leukemia or myelodysplastic syndrome. Similar to the oral suspension study1, prophylactic efficacy was assessed using a composite endpoint that included either confirmed/suspected invasive fungal infection, death, or the use of systemic antifungal therapy (patients may meet more than 1 criterion). This trial evaluated patients 7 days after the end of study treatment and 100 days after randomization to the group. The mean duration of treatment was similar between the 2 treatment groups (29 and 25 days in the posaconazole and fluconazole or itraconazole treatment groups, respectively). The results of Study 2 are shown in Table 9.
Table 9: Results of open clinical study 2 on oral suspensions for the prevention of invasive fungal infections in all patients with malignant hematologic disease and long-term neutropenia who received randomized subgroups
Posaconazole
Fluconazole/Itraconazole
n = 304
n = 298
< strong>7daysafter the end of treatment
< span style="font-family:Arial">Clinical Failure*†
82< span style="font-family:Arial">(27%)
126(42%)
Reason for failure:
After confirmed diagnosisSuspected invasive fungal infection
7 (2%)
25(< span style="font-family:Times New Roman">8%)
< td vAlign="middle" style="padding-left: 7px; padding-right: 7px; border-top: none; border-left: solid black 0.5pt; border-bottom: solid black 0.25pt; border-right: solid black 0.5pt"> (Aspergillus)
2(1%)
20(7%)
(Candida)
3(1%)
2 (1%)
(Other)
2 (1%)
< span style="font-family:Times New Roman">3 (1%)
< span style="font-size:10pt">All deaths
17(6%)
25(8< span style="font-family:Arial">%)
< span style="font-size:10pt">diagnosed before death/ “font-family:Arial”>suspected fungal infection
1(< 1< span style="font-family:Arial">%)
2(1%)
SAF‡
67(22%)
98(33%)
After random grouping 100 within
Clinical Failure†
158(52%)
191(64%)
Reason for failure:
< /td> Confirmed/suspected invasive fungal infection
14< span style="font-family:Arial">(5%)
33(11%)
(Aspergillus)
2(1%)
26(< span style="font-family:Times New Roman">9%)
< td vAlign="middle" style="padding-left: 7px; padding-right: 7px; border-top: none; border-left: solid black 0.5pt; border-bottom: solid black 0.25pt; border-right: solid black 0.5pt"> (Candida)
10(3%)
4 (1%)
(Other)
2(1%)
3 (1%)
All Dead
44< span style="font-family:Arial">(14%)
64(21%)
diagnosed before death/suspected fungal infection
2(1%)
16(5%)
SAF‡
98(< span style="font-family:Times New Roman">32%)
< p style="text-align: center">125(42%) No Incident Missed Visits§
< span style="font-family:Times New Roman">34(11%)
< span style="font-family:Times New Roman">24 (8%)
* 95% confidence interval (posaconazole-fluconazole/itraconazole) = (-22.9%, -7.8%).
† Patients may meet more than 1 failure definition criterion.
‡ Criteria for use of systemic antifungal therapy (SAF) as defined by the trial protocol (empirical/IFI use > 3 consecutive days).
§
Lost visits (not observed within 100 (not observed within days) and did not meet another clinical failure endpoint. These patients were considered to have failed.In summary, 2 prophylactic clinical studies of oral suspensions were conducted. As shown in the table (Tables 8 and 9), clinical failure was used as a composite end point, including breakthrough invasive fungal infection, death, and use of systemic antifungal therapy. In the oral mix study1 (Table 8), posaconazole (33%) had a similar rate of clinical failure to fluconazole (37%) (95% confidence interval for the posaconazole-control drug difference -11.5% to 3.7%). In contrast, in Oral Mix Study 2 (Table 9), the clinical failure rate was lower in patients treated with posaconazole (27%) than in those treated with fluconazole or itraconazole (42%) (95% confidence interval for the posaconazole-control drug difference -22.9% to -7.8%).
In the 2 treatment groups of the oral mix study 1, all-cause mortality at week 16 was similar [posaconazole 58/301 (19%) versus fluconazole 59/299 (20%)]; in the oral mix study 2, patients in the posaconazole-treated group had a lower all-cause mortality was lower than in the fluconazole/itraconazole-treated group [posaconazole 44/304 (14%) versus fluconazole/itraconazole 64/298 (21%)]. 2 studies demonstrated a lower incidence of breakthrough infections due to Aspergillus in patients receiving posaconazole prophylaxis than in patients receiving fluconazole or itraconazole treatment.
2. Posaconazole Oral Suspension for Oropharyngeal Candidiasis (OPC)
The Posaconazole Oral Suspension Study3 is a randomized, controlled, evaluator-blinded study in HIV-infected patients presenting with oropharyngeal candidiasis. Patients were treated with posaconazole or fluconazole oral suspension (posaconazole and fluconazole were administered as indicated below: 100 mg twice daily for 1 day, followed by 100 mg once daily for 13 days).
Clinical and fungal outcomes were evaluated after 14 days of treatment and at week 4 after the end of treatment. Patients who received at least 1 study drug and had positive oral swab cultures for Candida at baseline were included in the analysis (Table 10). The majority of subjects had a baseline phase pathogen of Candida albicans.
The rates of clinical success (complete or partial remission of all ulcers and/or plaques and symptoms) at day 14 and clinical relapse (recurrence of signs or symptoms after initial cure or improvement) at 4 weeks after the end of treatment were similar in the 2 treatment groups (Table 10).
The rates of fungal eradication (absence of colony-forming units in quantitative cultures on day 14 at the end of treatment) and fungal relapse (4 weeks after the end of treatment) were also similar in the 2 treatment groups (see Table 10).
Table 10: Clinical success, fungal eradication, and recurrence rates of posaconazole oral suspension in oropharyngeal candidiasis
Posaconazole
Fluconazole
clinical success rate at the end of treatment (day 14)
155/169(91.7%) >
148/160(92.5%)
Clinical Relapse rate (after the end of treatment4weeks)
45/155(29.0%)
52/148(< span style="font-family:Times New Roman">35.1%)
At the end of the treatment (day14days) fungal eradication rate (absence of CFU)
88/169< (52.1%)
80/160(50.0%)
Fungal recurrence rate (after the end of treatment< span style="font-family:Times New Roman">4weeks)
49/88(55.6%)
51/80(63.7%)
In the 2 treatment The fungal response rates were also similar in the groups (posaconazole 68.0%, fluconazole 68.1%), where the success criterion was a post-treatment quantitative culture with ≤ 20 colony-forming units (CFU/ml). The clinical significance of this result is unknown.
3. Posaconazole oral suspension for fluconazole- or itraconazole-refractory oropharyngeal candidiasis
The Posaconazole Oral Suspension Study4 is an uncontrolled study of Posaconazole oral suspension in HIV-infected patients presenting with fluconazole- or itraconazole-refractory oropharyngeal candidiasis. Oropharyngeal candidiasis was considered refractory if no improvement or exacerbation of oropharyngeal candidiasis was obtained after a standard course of fluconazole ≥100 mg daily for at least 10 consecutive days or itraconazole 200 mg daily for at least 10 consecutive days, and if fluconazole or itraconazole treatment was not discontinued more than 14 days before posaconazole treatment. Of the 199 subjects enrolled in this study, 89 met the strict criteria for refractory infection.
Forty-five subjects who developed refractory oropharyngeal candidiasis received posaconazole oral suspension 400 mg twice daily for 3 days, followed by 400 mg once daily for 25 days with an option to continue treatment for a 3-month maintenance period. After dose adjustment, an additional 44 subjects received posaconazole 400 mg twice daily for 28 days. The effectiveness of posaconazole was evaluated by clinical success (cure or improvement) rate after a 4-week treatment period. The clinical success rate was 74.2% (66/89). Clinical success rates were similar for the initial and modified dosing regimens (73.3% and 75.0%, respectively).
[Pharmacology and Toxicology
Pharmacological effects
Mechanism of action.
Posaconazole, a triazole antifungal, is a potent inhibitor of lanolin 14-demethylase, the catalytic enzyme for a key step in ergosterol biosynthesis. Posaconazole produces its antifungal effect by inhibiting lanolin 14-demethylase on the fungal cell membrane.
Microbiology.
In vitro tests and clinical infection studies have shown that posaconazole has antibacterial activity against the following microorganisms: Aspergillus spp. (Aspergillus fumigatus, Aspergillus flavus, Aspergillus terreus, Aspergillus oryzae, Aspergillus niger, Aspergillus pyogenes, Aspergillus ochraceus), Candida spp. (Candida albicans, Candida smoothus, Candida klebsiella, Candida subsmoothus), Cryptococcus neoformans, Clostridium vulgaris, Peptostreptococcus, Histoplasma intercalatum, Clostridium spp. Pseudoalicium bovis, Streptomyces spp, Ectoplasma spp, Fusarium spp, Dictyostelium spp, Trichoderma spp, Trichoderma spp and Rhizopus spp.
In vitro tests have shown that posaconazole also has antibacterial activity against the following yeasts and molds: Candida dublin, Candida saprophyticus, Candida quinquefaciens, Candida portugal, Candida lactis, Candida rugosa, Candida tropicalis, Candida salivarius, Candida ordinarius, Candida decidua, Candida norvegicans, Candida pseudotropicalis, Cryptococcus laurenti, Candida maxicruvii, Saccharomyces cerevisiae, Saccharomyces cerevisiae, Saccharomyces cerevisiae, Saccharomyces cerevisiae, Saccharomyces cerevisiae. Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon polysporon, Trichosporon fumigatus, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp, Trichosporon spp. However, there are no clinical trial studies on the safety and efficacy of posaconazole in the treatment of clinical infections caused by these microorganisms.
Posaconazole has broad-spectrum antifungal activity against yeasts and molds that do not respond to treatment with certain azoles or are resistant to other azoles.
- style=”margin-left: 38pt”>
-
Candida spp. (including isolates of Candida albicans resistant to fluconazole, voriconazole, and itraconazole (including Candida albicans isolates that are resistant to fluconazole, voriconazole, and itraconazole, Candida klebsiella and Candida smoothus that are not themselves susceptible to fluconazole treatment, and Candida portugal that is not itself susceptible to amphotericin B treatment)
- style=”margin-left: 38pt”>
-
Aspergillus spp. (including those sensitive to fluconazole, voriconazole, >itraconazole and amphotericin B resistant isolates)
- style=”margin-left: 38pt”>
-
Microorganisms previously identified as insensitive to azoles, such as jointed bacteria (e.g., Plasmodium spp., Trichoderma spp., Rhizopus spp. and Rhizopus spp.)
In vitro, posaconazole has bactericidal activity against the following genera.
- style=”margin-left: 38pt”>
-
Trichoderma spp.
- style=”margin-left: 38pt”>
-
Biphasic fungi (Bacillus dermatitidis, Histoplasma capsulatum, Penicillium marneffei, Coccidioides crassus)
-
Some Candida spp.
Posaconazole has shown antibacterial activity against a wide range of fungal infections caused by mycobacteria or yeasts in animal infection models. However, no consistent correlation was obtained between minimum inhibitory concentration values and effectiveness.
Before treatment, fungal culture specimens and other relevant laboratory studies (including histopathology) should be obtained to isolate and identify the causative microorganism. Treatment may be administered until fungal culture and other laboratory results are reported. However, once these results are available, antifungal treatment regimens should be adjusted accordingly.
Drug resistance.
In the laboratory, no posaconazole-resistant strains of Candida albicans were identified; the frequency of spontaneous mutations in experimental Aspergillus fumigatus with reduced susceptibility to posaconazole increased to 1×10-8 to 1×10-9. Clinically meaningful reductions in susceptibility to posaconazole by Candida albicans and Aspergillus fumigatus isolates are rare. In those rare cases of reduced susceptibility, no significant association was found between reduced susceptibility and clinical treatment failure. Posaconazole has been successful in the treatment of patients with microbial infections resistant to other azoles; also, in vitro posaconazole is active against Aspergillus and Candida strains resistant to other azoles and/or amphotericin B. The folding point for fungal therapy with posaconazole has not been established.
Combination therapy with antifungal drugs:
Posaconazole co-administration with amphotericin B or caspofungin was tested in vitro and in vivo, and no drug antagonism was seen, and in some cases additive drug effects were observed. The clinical significance of these results has not been determined.
Toxicological studies
Genotoxicity.
Posaconazole Ames test, human peripheral blood lymphocyte chromosome aberration test, Chinese hamster ovary cell chromosome aberration test, and mouse bone marrow micronucleus test results were negative.
Reproductive toxicity.
No effect on fertility was seen with posaconazole in male rats given a maximum dose of 180 mg/kg (exposure 1.7 times the oral suspension 400 mg twice daily dosing regimen at steady-state plasma concentrations in healthy volunteers) or in female rats given 45 mg/kg (exposure 2.2 times the oral suspension 400 mg twice daily dosing regimen).
In rats, posaconazole doses ≥ 27 mg/kg (≥ 1.4 times the steady-state plasma drug concentration of the oral suspension 400 mg twice daily dosing regimen in healthy subjects) resulted in skeletal deformities (cranial deformities and rib deficiencies). In rats, no skeletal deformities were observed at a dose (no effect dose) of 9 mg/kg (0.7 times the exposure of the oral suspension 400 mg twice daily dosing regimen). In rabbits, no deformities were observed at the maximum dose of 80 mg/kg. In rabbits, the no-effect dose was 20 mg/kg, while higher doses of 40 and 80 mg/kg resulted in increased embryonic uptake, with these doses producing exposure levels 2.9 or 5.2 times higher than the 400 mg twice daily dosing regimen, respectively. In rabbits, reduced body weight gain and reduced litter size were observed in females at the 80 mg/kg dose.
Reproductive, perinatal, and postnatal developmental studies were conducted in rats. Posaconazole caused skeletal abnormalities and malformations, obstructed labor, prolonged gestation, reduced mean litter size, and reduced postnatal viability when exposure was below the human therapeutic dose. In rabbit trials, posaconazole produced embryotoxicity at exposures above therapeutic doses. As with other azole antifungals, these reproductive effects were associated with administration affecting steroid hormone production.
Carcinogenicity.
No drug-associated tumors were observed in a 2-year carcinogenicity trial in rats or mice given higher than clinical doses of posaconazole. In a 2-year carcinogenicity trial in rats given posaconazole orally at a maximum dose of 20 mg/kg (females) or 30 mg/kg (males), these doses produced exposures that were 3.9 or 3.5 times higher, respectively, based on steady-state AUC in healthy volunteers consuming a high-fat diet (oral suspension 400 mg twice daily regimen). In the mouse test, the maximum dose administered orally was 60 mg/kg per day, and the exposure was 4.8 times that of the oral suspension 400 mg twice daily regimen.
Other.
As with other azole antifungals, posaconazole was found to have an inhibitory effect on steroid hormone synthesis in repeated dosing toxicity tests. Adrenal suppression was found in rat and canine toxicity tests at exposures at or above human therapeutic doses.
At dosing≥ 3months in a canine toxicity test, neuronal phospholipidosis was observed when the systemic exposure was less than the human therapeutic dose exposure. These changes were not observed in a monkey toxicity trial administered for 1year. In a neurotoxicity test in dogs and monkeys over a period of 12months, when systemic exposure was greater than human therapeutic dose exposure, no effects were observed on central or peripheral nervous system effects.
in rats over a period of2. span>year trial, pulmonary phospholipidosis leading to alveolar dilatation and obstruction could be observed. These results do not necessarily represent the potential for functional alterations in humans.
In safety pharmacology trials with repeated dosing in monkeys, when the maximum plasma concentration was the plasma concentration of the human therapeutic dose8.5fold, no effects on ECG were observed, including QTandQTc Interval. In a repeated administration safety pharmacology test in rats, when systemic exposure was 2.1fold of the human therapeutic dose exposure, echocardiographic cardiogram did not suggest cardiac decompensation. In rats and monkeys, when systemic exposure was 2.1fold and fold of the human therapeutic dose exposure, respectively style=”font-family:Times New Roman”>8.5fold, elevated systolic and arterial blood pressures were observed (29 mmHg).
[Pharmacokinetics].
Posaconazole is an azole antifungal drug.Dose-effect relationships: a wide range of posaconazole plasma exposure levels in clinical studies in neutropenic patients receiving cytotoxic chemotherapy for acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS) or in hematopoietic stem cell transplant (HSCT) recipients with graft-versus-host disease (GVHD). Pharmacokinetic-pharmacodynamic analysis of patient data showed a significant correlation between mean posaconazole concentrations (Cavg) and prophylactic effectiveness (Table 11). Lower Cav may be associated with an increased risk of treatment failure, i.e., discontinuation of therapy, use of empiric systemic antifungal therapy (SAF), or development of breakthrough invasive fungal infections.
Table 11: In Analysis of Posaconazole Oral Suspension Exposure in Prevention Clinical Trials (Cavg)
Preventive Applications in AML/MDS*
Preventive applications in graft-versus-host disease†
Cavg range (ng/ mL)
Treatment failure‡(%)
Cavg range (ng/mL)
Treatment failure‡ (%)
Quartile 1
90-322
54.7
22-557
44.4
Quartile 2
322-490
37.0
< span style="color:black; font-size:10pt">557-915
20.6
Quartile 3
490-734
46.8
915-1563
17.5
Quartile 4
td vAlign=”bottom” style=”padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: solid black 0.75pt; border- right: solid black 0.5pt”>
734-2200
27.8
< p style="text-align: center">1563-3650 17.5
Cavg = mean plasma concentration of posaconazole measured at steady state
*Neutropenic patients receiving cytotoxic chemotherapy for acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS)
†Hematopoietic stem cell transplant (HSCT) recipients with graft-versus-host disease (GVHD)
‡Defined as discontinuation of therapy, use of empiric systemic antifungal therapy (SAF), or development of breakthrough invasive fungal infection
General Pharmacokinetic Profile
The pharmacokinetics of posaconazole enteric-coated tablets after single and multiple doses up to 300 mg showed proportional to the dose administered. The mean pharmacokinetic parameters of posaconazole at steady state after administration of 300 mg twice daily (BID) on day 1 and once daily (QD) thereafter in healthy volunteers, neutropenic patients receiving cytotoxic chemotherapy for acute myeloid leukemia or myelodysplastic syndrome, or hematopoietic stem cell transplant recipients with graft-versus-host disease are shown in < strong>Table 12.
Table 12: Arithmetic mean (%CV) of steady-state pharmacokinetic parameters after administration of posaconazole enteric-coated tablets (300 mg)* in healthy volunteersand patients
< col style="width:61px"/> N
AUC0-24h (ng-hr/mL)
C avg† (ng/mL)
Cmax (ng/mL)
Cmin (ng/mL)
Tmax
‡(h)
t1/2
(h)
CL/F (L/h)
Healthy Volunteers
12
51618 (25)
2151 (25)
2764 (21)
1785 (29)
4 (3-6)
31 (40)
7.5 (26)< /p>
Patients
50
37900 (42)
< p style="text-align: center">1580 (42) 2090 (38)
1310 (50)
4 (1.3-8.3)
–
9.39 (45)
CV=coefficient of variation expressed as a percentage (%CV); AUC0-T=area under the plasma concentration-time curve from time zero to 24 hours; Cmax=highest observed plasma concentration; Cmin=lowest observed plasma concentration; Tmax=time to observe highest plasma concentration; t1/2=terminal segment half-life; CL/F=apparent overall clearance *300 mg twice daily on day 1 and 300 mg once daily thereafter †Cavg=time-averaged concentration (i.e., AUC0-24h/24 hours)‡median (min-max)
Absorption
:Oral administration in healthy volunteers of The medianTmax of absorption when posaconazole enteric-coated tablets are given orally is 4 to 5 h. Steady-state plasma concentrations are achieved by day 6 at a 300 mg dose (once daily, loading dose twice daily on day 1). The absolute bioavailability of oral enteric tablets was approximately 54% in the fasting situation. The Cmax and AUC of posaconazole were elevated by 16% and 51%, respectively, when posaconazole enteric tablets were administered concomitantly with a high-fat diet compared with the fasting situation (see Table 13). To enhance posaconazole absorption and optimize plasma concentrations, posaconazole enteric-coated tablets should be taken with food.
Table 13: Statistical comparison of the plasma pharmacokinetics of single oral administration of 300 mg posaconazole enteric-coated tablets in healthy subjects under fasting and feeding
Fasting
Eating
(High-fat diet)*
Feeding/Fasting
Pharmacokinetic parameters
N
Average (%CV)
N
Average (% CV)
GMR(90% CI)
Cmax (ng/mL)
14
935 (34)
16
1060 (25)
1.16 (0.96, 1.41)
AUC0-72hr(hr∙ng/mL)
14
26200 (28)
>
16
38400 (18)
1.51 (1.33, 1.72)
Tmax†(hr)
< p style="text-align: center">14 5.00
(3.00, 8.00)
16
6.00
(5.00, 24.00)
N/A
GMR = geometric least squares mean ratio; CI = confidence interval
* 48.5 g fat
† Tmax mean (min, max)
>
Posaconazole enteric-coated tablets did not show a significant effect on posaconazole pharmacokinetic exposure dose when administered concomitantly with drugs affecting gastric pH or gastric motility (seeTable 14).
Table 14: Effect of concomitant administration of drugs affecting gastric pH and gastric motility on the pharmacokinetics of posaconazole enteric tablets in healthy volunteers
Medications given at the same time
>
Dosing group
Cmax changes
(ratio estimate*; ratio estimate 90% confidence interval)
AUC0-last change
(ratio estimate*; ratio estimate 90% confidence interval)
Mylanta® High Efficiency Solution
(Raises gastric pH)
25.4 milliequivalents (meq)/5mL, 20mL
↑6%
(1.06; 0.90 -1.26)↑
↑4%
(1.04; 0.90 -1.20)
Renitidine (Zantac®)
(Alters gastric pH)
150mg (150mg of ranitidine given in the morning, twice daily)
↑4%
(1.04; 0.88 -1.23)↑
↓3%
(0.97; 0.84 -1.12)
Esomeprazole (Nexium®)
(Raise gastric pH)
40mg (5 days of morning dosing, day -4 to day 1)
↑2%
(1.02; 0.88-1.17)↑
↑5%
(1.05; 0.89 -1.24)
Metoclopramide (Reglan®)
(Increase gastric power)
15mg 4x daily for 2 days (day -1 and day 1)
↓14%
(0.86, 0.73,1.02)
↓7%
(0.93, 0.803,1.07)
*Ratio estimated as C for concurrent administration of drug plus posaconazole versus posaconazole alone max or AUC0-last ratio
Distribution: The mean volume of distribution of posaconazole after intravenous administration of posaconazole in healthy volunteers was 261 L, with a range between 226-295 L across trials and doses.
Metabolism.
Posaconazole is present in the plasma primarily as the parent drug. Of the circulating metabolites, the majority are glucuronide conjugates formed via UDP glucosylation (2-phase enzyme). Posaconazole does not produce any major circulating oxidative (CYP450-mediated) metabolites. Metabolites excreted in urine and feces account for approximately 17% of the radiolabeled dose.
Posaconazole is metabolized primarily by UDP glucosylation (2-phase enzyme) and is a substrate for p-glycoprotein (P-gp) pump-out action. Therefore, inhibitors or inducers of these clearance pathways can have an impact on posaconazole plasma concentrations. A summary of clinical studies of oral suspensions or early tablet prescriptions that could have an effect on posaconazole concentrations can be found in Table 15.
Table 15: Summary of Effects of Combinations on Posaconazole in Healthy Volunteers
Combination drugs
(Assumed Mechanism of Interaction)
< strong>Combination drug dose/ scheme
Posaconazole dosing/Protocol
Effect on posaconazole bioavailability
averageCmax< strong>of change (estimated ratio*; estimated ratio of90% confidence interval)
AverageAUCVariation (estimated ratio*; estimated ratio of90% confidence interval)
Following the law, Veronica
(UDP-Ginduction )400 mg(oral suspension) daily2times × 10days and20 span>Ten
< span style="font-family:Times New Roman; font-size:9pt">↓45%
(0.55;0.47- 0.66)
↓ 50%
(0.50;0.43- 0.60)
Fosamprenavir
(the rationale is unclear)
700mg twice daily for 10 days
200mg once daily on day 1, 200mg twice daily on day 2, then 400mg twice daily x 8 days
td vAlign=”middle” style=”padding-left: 7px; padding-right: 7px; border-top: none; border-left: none; border-bottom: solid black 0.75pt; border- right: solid black 0.5pt”>
↓21%
0.79 (0.71-0.89)
↓23%
0.77 (0.68-0.87)
Rifabutin
(UDP-Ginduction)
300 mgdaily1timedaily × 17days
200 mg(tablet) daily1time × 10days†
↓ 43%
(0.57;0.43- 0.75)
↓ 49%
(0.51;0.37- 0.71)
Phenytoin
((UDP-Ginduction)
200 mgdaily1timedaily × 10days
200 mg(tablet) daily1time × 10days†
↓ 41%
(0.59;0.44- 0.79)
↓ 50%
(0.50;0.36- 0.71)
*The estimated ratio is the ratio of Cmax or AUC of the combination drug plus posaconazole to posaconazole monotherapy.
†The tablets used are non-commercialized tablet formulations without polymers.
In vitro and clinical studies on human liver microsomes have shown that posaconazole is primarily aCYP3A4inhibitor. Clinical studies in healthy volunteer subjects have also shown posaconazole to be a potentCYP3A4inhibitor, with evidence for midazolam’s /span>AUCelevated5fold or more. Thus, posaconazole can lead to increased plasma concentrations of drugs that are metabolized primarily via CYP3A4. A summary of the drugs whose plasma concentrations were affected by posaconazole in clinical studies can be found in Table16.
Table 16: Summary of the effect of posaconazole on co-administration in healthy volunteers and patients
Combination of drugs
(assuming the mechanism of interaction is posaconazole inhibitionCYP3A4)
Combination drug dose/Protocol
Posaconazole dose/Protocol
Effect on bioavailability of co-administered drugs
AverageCmaxvariation (estimated ratio*; estimated ratio of90% confidence interval)
AverageAUC< span style="font-family:Arial">variation (estimated ratio*; estimated ratio of90% confidence interval)
Sirolimus< span style="font-family:Times New Roman">
2 mgSingle oral dose
400 mg(oral suspension) daily2times × 16day
↑ 572%
(6.72;5.62- 8.03)
↑ 788%
(8.88;7.26- 10.9)
Cyclosporine
Stable maintenance received by heart transplant patients Dose
200 mg< (tablet)daily1< span style="color:black">time
× 10days↑ Cyclosporine whole blood trough concentration
Cyclosporine needs to be 29%
Tacrolimus
0.05 mg/kgsingle oral dose
< span style="font-size:10pt">400 mg(oral suspension) daily2times × 7< span style="font-family:Arial">day
↑ 121%
(2.21;2.01- 2.42)
↑ 358%
(4.58;4.03- 5.19)
Simvastatin
40 mgSingle oral dose
100 mg(oral suspension)daily >1timesa day
× 13days200 mg(oral suspension)daily1time
× 13daysSimvastatin
↑ 841%
(9.41,7.13- 12.44)
Simvastatin acid
↑ 817%
(9.17,7.36 – 11.43)
Simvastatin
↑ 1041%
(11.41,7.99-16.29)
Simvastatin acid
↑ 851%
(9.51,8.15- 11.10)
Simvastatin
↑ 931%
(10.31,8.40- 12.67)
Simvastatin acid
↑ 634%
(7.34,5.82 – 9.25)
Simvastatin
↑ 960%
(10.60,8.63 – 13.02)
Simvastatin acid
↑ 748%
(8.48,7.04 – 10.23)
< span style="font-family:Arial">midazolam
0.4 mg< /span>Single intravenous dose‡
0.4 mgsingle intravenous dose‡‡ =”font-size:10pt”>
2 mgsingle oral dose‡
2 mgsingle oral dose‡
200 mg< /span>(oral suspension) daily2times × 7days
400 mg(oral suspension) daily2times × 7days
200 mg(oral suspension)daily1time
× 7days400 mg(oral suspension) daily2times × 7days
↑ 30%
(1.3;1.13- 1.48)
↑62%
(1.62;1.41- 1.86)
↑ 169%
(2.69;2.46- 2.93)
↑ 138%
(2.38;2.13- 2.66)
↑ 362%
(4.62;4.02- 5.3)
↑524%
(6.24;5.43- 7.16)
↑ 470%
(5.70;4.82- 6.74)
↑ 397%
(4.97;4.46- 5.54)
Rifabutin
300 mg< /span>daily1times
× 17days200 mg< (tablet)daily1< span style="color:black">time
× 10daysdays†↑ 31%
(1.31;1.10- 1.57)
↑ 72%
(1.72;1.51- 1.95)
Phenytoin
200 mg< /span>daily1timesoral administration × 10day
200 mg< (tablet)daily1< span style="color:black">time
× 10daysdays†↑ 16%
(1.16;0.85- 1.57)
↑ 16%
(1.16;0.84- 1.59)
Ritonavir
100 mg< /span>daily1times
× 14days400 mg< /span>(oral suspension) daily2times × 7days
↑ 49%
(1.49;1.04- 2.15)
↑ 80%
(1.8;1.39-2.31)
Azanavir
Atazanavir/Ritonavir add-on therapy
300 mgdaily1time
× 14days300 mg/100 mgdaily1time
× 14days400 mg(oral suspension) daily2times. family:Times New Roman”> × 7days
400 mg(oral suspension) daily2times × 7days
↑ 155%
(2.55;1.89-3.45)↑ 53%
(1.53;1.13- 2.07)
↑ 268%
(3.68;2.89- 4.70)
↑ 146%
(2.46;1.93- 3.13)
< span style="font-size:10pt">* The estimated ratio is the ratio of Cmax or AUC of the combination drug plus posaconazole to the combination drug monotherapy.
† The tablets used are non-commercialized tablet formulations without polymers.
† The mean terminal half-life of midazolam was extended from 3 hours to 7 to 11 hours during combination therapy with posaconazole.
Other clinical studies have demonstrated no clinically significant effects of zidovudine, lamivudine, indinavir, or caffeine when combined with posaconazole 200 mg once-daily regimen. Therefore, no dose adjustment is required for these drugs when combined with the posaconazole 200 mg once-daily regimen.
Excretion:
Posaconazole is primarily cleared via the feces (71% of the radiolabeled amount at 120 hours), with the major portion of clearance being the prodrug (66% of the radiolabeled amount). Renal clearance is the secondary route of clearance, with 13% of the radioisotope labeled amount excreted in the urine (of which <0.2% of the radiolabeled amount is prodrug).
The mean half-life (t1/2) for clearance of posaconazole enteric-coated tablets ranged from 26 to 31 hours.
[Storage].
Store at 20°C -25°C with a permissible deviation of 15°C -30°C.
[Packaging
This 100 mg enteric coated tablet is packaged in a polyvinyl chloride (PVC)/polyvinyl chloride trifluoride film blister with a pressed-in aluminum foil closure.
24 tablets/box
[Expiration date]24 months
[Executive Standard].
JX20160196
[Approval Number].
[Manufacturer].
Company name: Merck Sharp & Dohme Ltd
Address: Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, United Kingdom
Manufacturer’s name: N.V. Organon
Address: Kloosterstraat 6, 5349 AB Oss, The Netherlands
Name of packaging plant: Schering-Plough Labo N.V.
Address: Industriepark 30, Heist-op-den-Berg, 2220, Belgium
In-country contact.
Tel: 021-22118888
Fax: 021-22118899
-