In recent years, what has really put immunotherapy on the cancer treatment scene is the successful use of immune checkpoint inhibitors.
What is an immune checkpoint inhibitor?
Checkpoints are a set of molecules expressed on immune cells that regulate the degree of immune activation and play an important role in preventing autoimmunity (abnormal immune function that attacks normal cells) from occurring. The tumor cells use this mechanism to “exploit” and suppress the immune cells, so that these “body police” are not working, and they can escape surveillance and survive.
The common immune checkpoints are CTLA-4 (cytotoxic T lymphocyte-associated antigen-4), PD-1 (programmed death-1), and others. They are all a protein (receptor) on the surface of T lymphocytes.
Tumor cells express substances to activate immune checkpoints. Once the latter is activated, it acts as a “brake” that prevents antigen presentation to T cells, blocking the antigen presentation process in the tumor immune loop and thus suppressing T cell immune function.
And immune checkpoint inhibitors are suppressive drugs developed to target the immune checkpoint, allowing the immune cells to rejuvenate and re-eliminate cancer cells. They have been marketed both domestically and internationally.
What are the effects of immune checkpoint inhibitors?
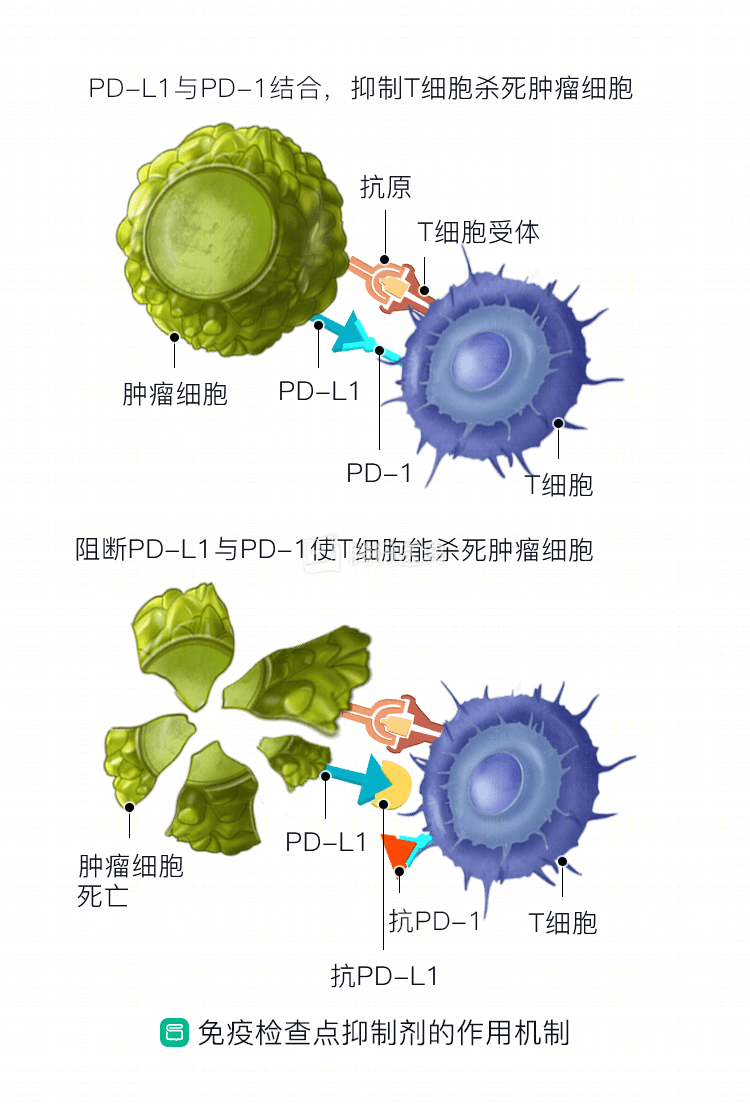
Immune checkpoint inhibitors block the binding of inhibitory immune checkpoints such as PD-1 and CTLA-4 to their corresponding ligands, “unlocking” the function of T cells and “waking” them up to recognize and kill tumor cells.
Let’s take PD-1/PD-L1 inhibitors as an example: PD-1 is a protein that is distributed on the surface of lymphocytes and inhibits the action of immune cells. This is an “internal defense system” that prevents the immune system from killing its own cells, but tumor cells can express a substance called PD-L1, which binds to PD-1 and initiates a process of lymphocyte “inactivation” to escape the immune system. “PD-1/PD-L1 inhibitors interrupt this chain.
How well do immune checkpoint inhibitors work?
The data show that pembrolizumab (Pembrolizumab), nabolutumab (Nivolumab), and the new drugs developed in China, SHR-1210 and JS001, have an efficiency rate of 17%, 28%, 46.7%, and 23.5%, respectively, in esophageal cancer. Of these, patients who respond to treatment are expected to survive long-term, but there is still a large portion of the population that will not benefit.
In a phase I/II clinical trial, investigators used nabolutumab , alone or in combination with epirimizumab, to treat patients with advanced gastric, esophageal, and esophagogastric junction cancers who had failed prior chemotherapy. The results showed a 14% remission rate and a 35% 1-year survival rate in the nabumetumab monotherapy group.
Another clinical study, KETNOTE-012, in PD-L1-positive patients who had failed multiple treatments and were treated with pabrolizumab monotherapy, had a remission rate of 22%, median survival 11 months, and tolerable adverse effects.
In 2016, the American Society of Clinical Oncology (ASCO) annual meeting reported the results of a phase I clinical study called KETNOTE-028, which showed a 30% remission rate with pembrolizumab for PD-L1 expression-positive, multiple-treatment-failed esophageal cancer. The remission rates for squamous and adenocarcinoma were 29% and 40%, respectively.
Can I use an immune checkpoint inhibitor?
At this time, immune checkpoint inhibitors are not approved for use in the treatment of esophageal cancer. For you to be treated with an immune checkpoint inhibitor, you will need to participate in an appropriate clinical trial.
In general, people who cannot participate in clinical trials include:
- Patients with autoimmune diseases;
- Patients infected with hepatitis B, C, or HIV;
- Patients with interstitial pneumonia;
- Patients with a history of other tumors;
- Pregnant women, lactating women, etc.
In addition, your doctor will evaluate your medical condition and qualify you for the clinical trial.
In short, your ability to use immunotherapy requires guidance and advice from your doctor.
If I can participate in a clinical trial, how long will the treatment take?
The duration of dosing for immunotherapy is determined by several things.
In China, there are more than a dozen anti-PD-1/PD-L1 clinical trials related to esophageal cancer, and the duration of dosing needs to be given according to the different types of inhibitors, the regulations of the different clinical trials, and the time to emergence of the immune response.
The response time for immune checkpoint inhibitors is slow, with a response likely to occur after at least two months of treatment. In the absence of significant side effects, continuous dosing is required.
If you have an adverse reaction, your doctor will take steps to manage it; serious adverse reactions will be stopped.
Is immunotherapy expensive?
If you can participate in a clinical trial, there is no cost to purchase the drug. More than a dozen PD-1/PD-L1 inhibitors developed by our local drug companies are already in clinical studies and will be more affordable if they are approved for marketing.
What to look for during treatment?
If you can have immunotherapy, you need to cooperate with your doctor and not take medications that have not been approved by your doctor, which could interfere with the efficacy and your doctor’s judgment. You also need to monitor your health and report any discomfort to your primary care provider immediately.
Co-written by:
Dr. Jiao Xi, Department of Gastrointestinal Oncology, Peking University Cancer Hospital