Suspected of esophageal cancer, doctors prescribed gastroscopy, many people will wonder: why do we need to do gastroscopy when we are obviously looking for lesions in the esophagus? The first thing you need to do is to get a gastroscopy.
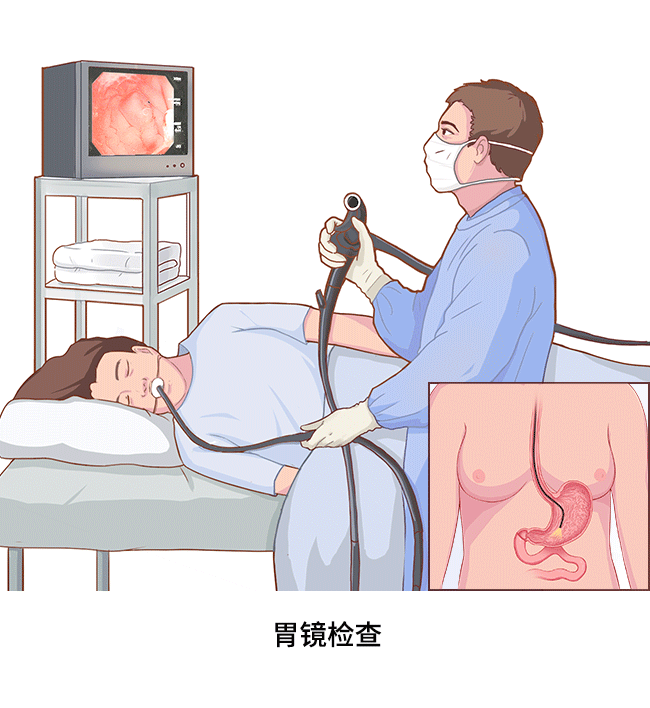
In fact, electronic gastroscopy is an important diagnostic method for esophageal cancer, in which a miniature camera “videos” your esophagus and stomach and displays them clearly on a monitor for your doctor to see.
Esophagoscopy is a device that doctors rarely use to diagnose esophageal cancer, although it is available. This is because when a tumor occurs in the lower esophagus, especially if the lesion invades the stomach or occurs in the combination of the esophagus and stomach, the esophagoscope cannot visualize the gastric lesion.
What preparation is needed before gastroscopy?
1. Fast for at least 6 hours. It is important to keep the esophagus and stomach clean and free of food debris during gastroscopy to ensure clear visualization of lesions on the esophageal mucosa.
2. Barium contrast (“barium meal”) should not be performed until at least 3 days after gastroscopy. This is because the barium adheres to the esophageal and gastric mucosa, especially in the ulcer area, which can interfere with the doctor’s observation and judgment.
3. Gastroscopy is an invasive test, so blood must be drawn for infection screening (hepatitis, syphilis, HIV, etc.) and blood tests, coagulation, etc., before gastroscopy is done.
What is the gastroscopy procedure like, and does it hurt?
1. To reduce your salivation, you will be given atropine 15-30 minutes before the procedure; if you are too nervous, you will be given 5-10 mg of Valium and given a lidocaine syrup for local anesthesia and lubrication.
2. During the exam, you lie on your side on the exam table with your legs bent, take the mouth pad and gently bite down on it. The doctor stands about 20 cm in front of your body, holding the mouthpiece in his or her left hand and the gastroscope in his or her right hand. At the beginning of the procedure, you breathe deeply through your nose, without moving your head, and relax your entire body as the gastroscope passes through the mouthpiece and into your mouth. When the gastroscope reaches the pharynx, you need to swallow so that the gastroscope can pass smoothly through the pharynx. You should not swallow during the gastroscopy, but allow the saliva to flow from the mouth pad into the curved tray.
3. If a lesion is found during the exam, a biopsy will be required. The doctor will use a biopsy forceps to remove the lesion and place it in a 10% formalin solution to fix and send it for examination.
To learn more about pathologic biopsy, read the following articles:
4. If the esophageal mucosa shows diffuse roughness and unevenness and the physician is unable to detect the lesion by visual observation, endoscopic staining is required. A small amount of dye is attached to the suspected lesion to be observed by oral, spray, or direct injection to make the color contrast between the lesion and the normal mucosa more obvious, helping the physician to identify the lesion and accurately remove the biopsy tissue.
Toluidine blue staining is based on the principle that tumor cells are richer in DNA than normal cells, and their cellular spaces are larger than normal cells, so the dye penetrates more easily into the tumor cell, causing its nucleus to stain blue; whereas normal esophageal epithelium is not stained. In this way, tumor cells are specially marked and can be easily detected.
The principle of iodine solution staining is that normal esophageal squamous epithelial cells contain glycogen, which appears brown when exposed to iodine. The epithelium that is cancerous has lost glycogen and does not stain when exposed to iodine, thus distinguishing it from normal epithelium.
How long does a gastroscopy usually take?
The full examination can usually be completed in 10 minutes.
If a lesion is found that requires an additional biopsy, it may take longer, but it can usually be done in 20-30 minutes.
Who should not have a gastroscopy?
While gastroscopy continues to improve in comfort, it is still an invasive procedure that not everyone can tolerate.
1. As a screening tool, gastroscopy is only recommended for people at high risk (pictured below).
2. Patients who require careful evaluation by a physician for electrogastroscopy: (1) cardiopulmonary insufficiency; (2) gastrointestinal bleeding; (3) severe hypertension, fluctuating or unstable blood pressure; (4) severe bleeding tendency with hemoglobin below 50 g/L or prothrombin time (PT) prolongation of more than 1.5 seconds; and (5) high spinal deformity.
3. Patients who cannot undergo electrogastroscopy: (1) severe cardiopulmonary disease; (2) suspected critical illness such as shock or perforation of the gastrointestinal tract; (3) mental illness and inability to cooperate with the examination; (4) acute inflammation of the gastrointestinal tract (acute gastritis, enteritis, etc.), especially corrosive inflammation; (5) significant thoracoabdominal aortic aneurysm; and (6) stroke.
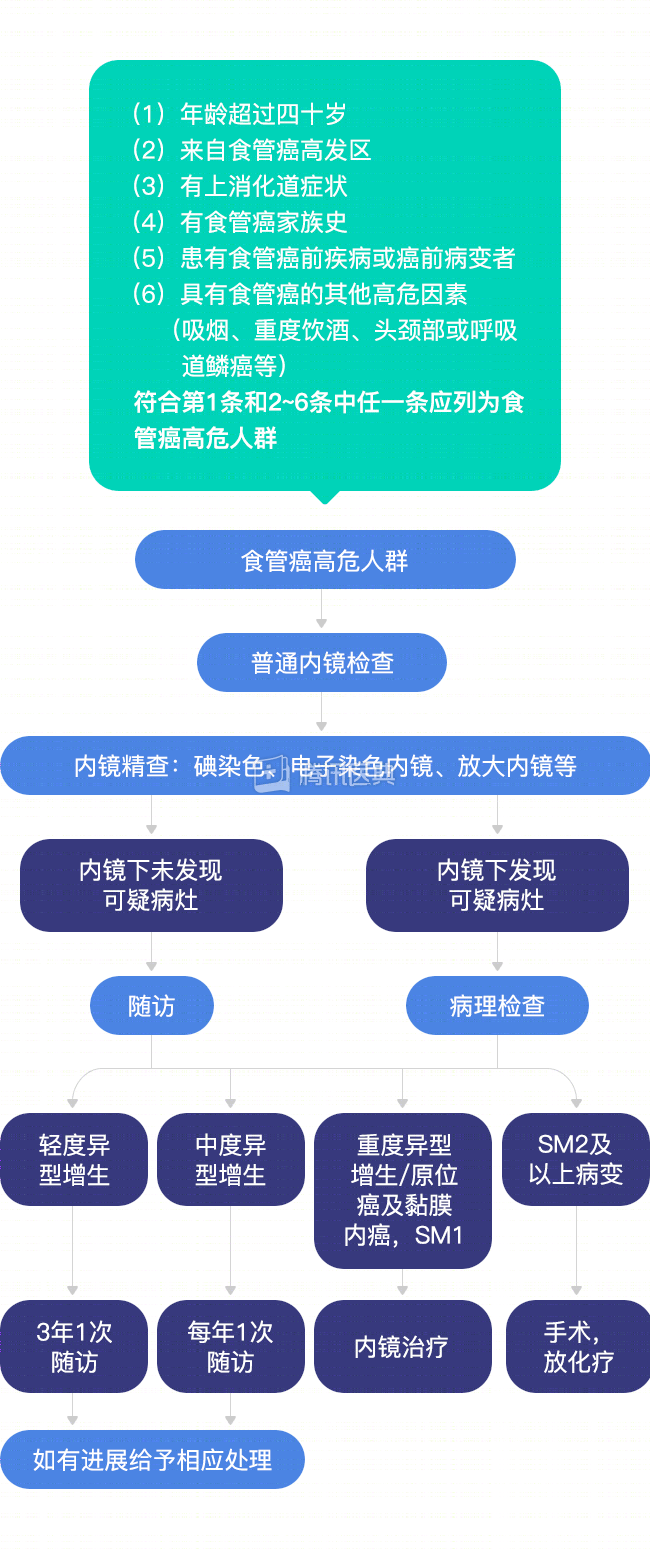
Early esophageal cancer screening and endoscopic precision flow chart
Note: SM1 is the upper 1/3 layer of the lesion infiltrating the submucosa; SM2 is the middle 1/3 layer of the lesion infiltrating the submucosa
How does the physician make the initial diagnosis based on what is seen microscopically?
In early-stage esophageal cancer, the lesion is confined to the mucosal surface and microscopically visible as congestion, erosion, plaques, or papillary lesions without a definite mass.
In intermediate and advanced esophageal cancer, the tumor grows and forms a mass, and a prominent mass, deep ulcer and narrowing of the esophageal lumen are seen microscopically.
But what is seen on gastroscopy still cannot accurately determine the early or late stage of the disease. This is because gastroscopy cannot see the depth of mass infiltration, but only intraesophageal manifestations such as neoplasia (below). The exact staging still requires a pathological biopsy to be taken for diagnosis.
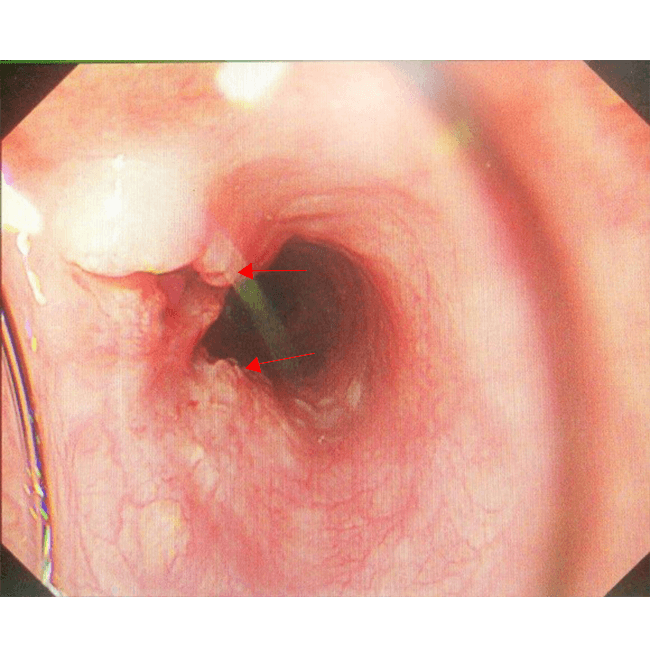
Gastroscopy shows an ulcerated neoplasm with elevated margins on the right anterior wall of the esophagus.
What to look for after gastroscopy?
1. Patients who do not need a biopsy can eat about 30 minutes after the postoperative oropharyngeal anesthetic wears off; patients who need a biopsy should not eat a warm, cool, liquid diet (warm milk, cool milk, warm rice porridge, etc.) until 2 hours after the procedure to reduce friction on the traumatized surface of the gastric mucosa.
2. There may be discomfort or pain in the throat or hoarseness after surgery, which usually improves within a short period of time and does not require stress. You can gargle light saline or take throat tablets to reduce symptoms. If there is active bleeding, such as vomiting blood, blood in the stool, and changes in heart rate, blood pressure, and other vital signs, be sure to report to your doctor immediately and do the appropriate treatment in a timely manner.