In China, lung cancer has the highest incidence and mortality rate of all cancers. The National Cancer Center survey showed that in 2015, there were about 787,000 new cases of lung cancer in China, with an incidence rate of 57.26 per 100,000.
According to pathological histology, lung cancer can be divided into two categories: small cell lung cancer and non-small cell lung cancer (NSCLC). The latter is the most common type, accounting for 85% of all lung cancers, and its 5-year survival rate is only 16%.
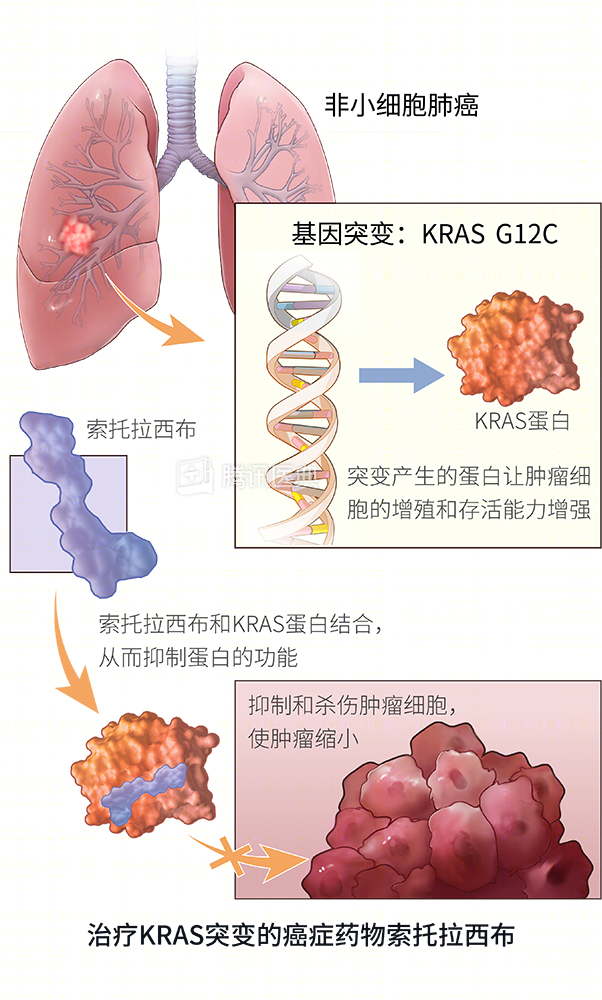
A key target for treating non-small cell lung cancer is the KRAS gene. However, the scientific community has been trying for more than 30 years to find a drug to “break” it. Until recently, a targeted drug called sotolacib came out of the woodwork, and its phase 2 clinical trial results were published in the New England Journal of Medicine, the world’s top medical journal.
Tackling the thief, how to break the KRAS gene?
How can we break the KRAS gene?
Cancer is often accompanied by thousands of genetic mutations, and only a few of these genes, called “driver genes,” are the main protagonists of this cellular “mutiny.
KRAS is an important gene.
KRAS is an important driver gene and is the most frequently mutated oncogene in human cancers. KRAS mutations have also been associated with resistance to targeted therapies and poor outcomes.
To catch a thief, it is these driver genes that are the drug targets of targeted cancer therapies. By identifying tumor cells that carry such mutated driver genes, targeted drugs can block signaling pathways, inhibit and kill tumor cells with greater precision and fewer side effects than traditional radiotherapy, and can significantly extend the survival of patients with advanced non-small cell lung cancer.
Despite more than 30 years of scientific effort, the lack of an obvious structure on the surface of the KRAS protein that can bind to drug molecules has left the drug “untouched”. It’s no wonder that scientists have reluctantly called it the “incurable” driver gene, knowing who the “leader” of the rebellion is, but you can’t break it.
Finally, the world’s first cancer drug for KRAS mutations, sotolacib, was born, giving the long-dormant drug development industry a shot in the arm. The scientists found an inconspicuous surface groove on the KRAS protein, and sotolacib was able to bind to it, controlling the “big brother” and quelling the “rebellious” momentum of the cancer cells. And this action is irreversible, which makes the drug more potent and selective.
Phase 2 clinical trial, 80% of patients’ tumors shrink
Following promising results from the phase 1 clinical trial, the phase 2 trial continues to explore the efficacy and safety of sotolacib monotherapy in patients with locally advanced or metastatic KRAS p.G12C mutated non-small cell lung cancer.
Specifically, this trial enrolled 128 patients with locally advanced or metastatic non-small cell lung cancer who carried the KRAS p.G12C mutation and had received chemotherapy or chemotherapy in combination with immunotherapy. Patients received sotolacib once daily by mouth at 960 mg. Dosing continued until disease progression occurred, unacceptable side effects occurred, or patients withdrew informed consent.
The median duration of treatment for these patients was 5.5 months as of March 15, 2021. The researchers assessed tumor remission by contrast-enhanced CT or MRI and found an objective remission rate of 37.1%, a median duration of remission of 11.1 months, a median progression-free survival of 6.8 months, and a median overall survival of 12.5 months. In addition, the majority of patients (80.6%) achieved tumor shrinkage and disease control.
In terms of safety, treatment-related adverse events occurred in 88 of 126 patients (69.8%), of which 26 were more serious grade 3 events (19.8%) or grade 4 events (0.8%). The most common adverse events included diarrhea, nausea, fatigue, and elevated alanine aminotransferase or aspartate aminotransferase levels.
In this phase 2 trial, sotolacib resulted in a durable clinical benefit with no new safety signals. Meanwhile, a phase 3 trial comparing sotolacib with chemotherapy is underway. Today, sotolacib is the first target drug approved by the FDA for the second-line treatment of KRAS gene mutations in non-small cell lung cancer.
Translating complex genetic information into actionable cancer treatment options, precision medicine offers hope for long-term survival of patients with advanced cancer.