Many people go to the doctor because of difficulty swallowing, throat or chest discomfort, and the test results show “severe atypical hyperplasia of the squamous epithelium” or even “carcinoma in situ of the esophagus”. What does this mean?
These are complicated medical terms.
These complex medical terms represent several stages of esophageal cancer development.
Esophageal cancer generally progresses through a “three-step” process of precancerous lesions (atypical epithelial hyperplasia), carcinoma in situ, and invasive carcinoma. Here is a brief overview.
1. precancerous lesions
The precancerous lesions of esophageal cancer can be classified as atypical hyperplasia and columnar epithelial metaplasia of the esophageal mucosa.
What is atypical hyperplasia of the esophageal mucosa?
What is atypical hyperplasia of the esophageal mucosa?
Atypical hyperplasia is medically defined as a loss of normal cell morphology with early manifestations of mutations, often occurring in people with chronic injury to the esophageal mucosa and chronic esophagitis.
People who love to eat hot porridge, drink excessively hot food such as work tea, and chew betel nut and tobacco are subject to repeated damage to the esophageal mucosa and are in a chronic state of inflammation for a long time. The mucosa will develop atypical hyperplasia during the vicious cycle of repeated injury-repair-reinjury-repair.
In most cases, severe atypical hyperplasia of the esophageal mucosa is treated as a “precancerous lesion,” which means that if it progresses further, it is an early stage cancer.
While severe atypical hyperplasia is one step away from carcinoma in situ, it is an extremely slow process that can take years to a decade to develop. For some people, it will not develop into in situ cancer in their lifetime.
But after a diagnosis of severe atypical hyperplasia, you still need to have frequent follow-up gastroscopies to detect the cancer early and treat it as soon as it is detected.
What is columnar cell metaplasia?
The inner surface of the normal esophagus is covered with “squamous epithelium”, whereas the stomach, to which the lower esophagus is attached, is covered with “columnar epithelium”.
Some people have a condition called gastroesophageal reflux disease (also known as reflux esophagitis), which causes food from the stomach and acidic gastric juices to flow backwards into the esophagus, causing the “squamous epithelium” of the lower esophagus to become “columnar epithelium” over time. This process is known as “columnar epithelium”. This process is medically known as epithelial metaplasia, and the esophagus in which this change occurs is called “Barrett’s esophagus” (Barrett’s esophagus).
This process is often accompanied by atypical hyperplasia; Barrett’s esophagus itself is a benign lesion, but studies have shown that about 10% of patients with Barrett’s esophagus may develop esophageal cancer, hence the term “precancerous lesion.
It is important to note that most cases of Barrett’s esophagus result in esophageal adenocarcinoma. Studies have shown that patients with Barrett’s esophagus have a 20-fold higher risk of adenocarcinoma than the normal population. However, this disease is uncommon in China, where data show that its prevalence is about 0.06% to 1%; it is common in Western whites, where the prevalence is about 1.6% to 6.8%. This may explain why so few of the patients with esophageal cancer in China are adenocarcinoma (only about 10%).
If you have frequent symptoms such as acid reflux and heartburn, go to the hospital to be checked for reflux esophagitis or Barrett’s esophagus and follow your doctor’s instructions for aggressive treatment.
.
2. Carcinoma in situ
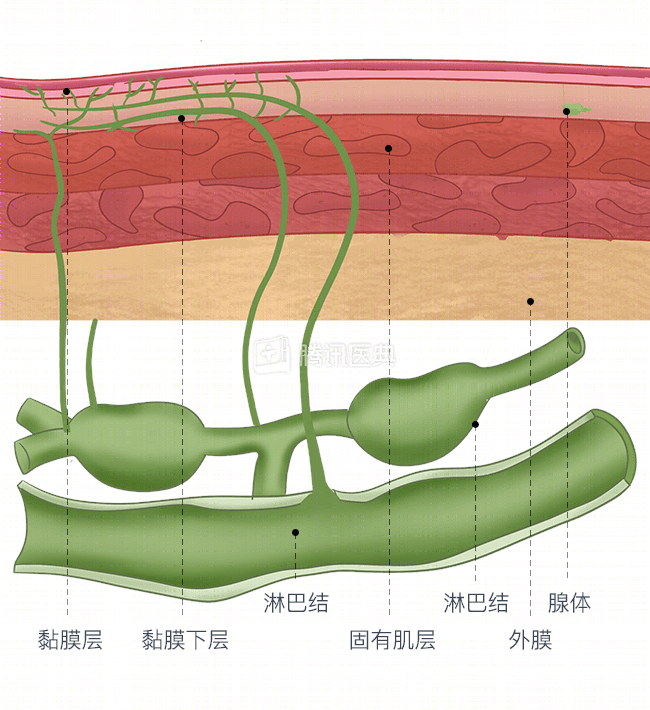
Esophageal cancer progresses “from superficial to deep”. The esophageal wall has 4 layers: mucosa, submucosa, lamina propria, and epithelium (see figure). When the cancer is confined to the mucosal epithelium and does not break through the basement membrane, it is called carcinoma in situ, which is the early stage of esophageal cancer.
So, what do we mean by “lesion confinement”? Here’s an analogy with a banana:
- An unripe banana with a smooth surface and no black spots is like a healthy esophagus;
- When the banana starts to ripen, the surface turns from green to yellow and there are some black spots, but the flesh is still good when you peel the skin off, it is like a cancer in situ, the “cancer cells” have not yet spread to the inside of the body;
- When the banana is “ripe”, the surface turns from green to yellow and there are some black spots.
- When the banana is “ripe” and the flesh is black and soft, it is like the cancer cells have spread to a deeper level, which is the “invasive cancer” we will talk about below.
In the stage of carcinoma in situ, there are usually no obvious symptoms, and most are detected during gastroscopy.
Therefore, if you have risk factors for esophageal cancer, regular endoscopic screening is recommended as an important means of detecting carcinoma in situ. Once detected, carcinoma in situ should be treated as soon as possible and in most cases can be cured by endoscopic resection, with a 5-year survival rate of 85% to 90%. Moreover, carcinoma in situ does not metastasize. If not treated in a timely manner, carcinoma in situ can develop into invasive cancer, which can be life-threatening.
3. invasive carcinoma
In situ carcinoma progresses further down the line to invasive carcinoma, which means “banana meat has gone bad”. You will slowly develop some clinical symptoms, such as difficulty swallowing, vague pain behind the sternum, hoarseness, etc.
Infiltrating cancer has the potential to metastasize and spread. It may invade deeper into the esophagus and even “invade” organs around the esophagus, such as the trachea, pleura, or pericardium, or metastasize to lymph nodes, liver, lungs, and other organs.
It is important to note that the progression from healthy esophagus to precancerous lesions and then to carcinoma in situ is very slow, and the progression time is measured in years, and it takes many years to progress one step. However, after the development of invasive cancer, the cancer progression is gradually accelerated and the development rate is measured in months.