Leptomeningeal metastasis (LM) is the diffuse metastasis of malignant tumor cells in the subarachnoid space of the brain and spinal cord and is one of the serious complications of advanced non-small cell lung cancer (NSCLC). Currently, the literature reports that approximately 3%-5% of patients with advanced NSCLC develop meningeal metastases. Among NSCLC patients diagnosed with LM, lung adenocarcinoma is the most common pathological type, accounting for approximately 84% to 97%, while lung squamous carcinoma accounts for only 1% to 6%.
The diagnosis of LM is difficult, and physicians currently rely on a combination of clinical presentation, cerebrospinal fluid (CSF), and imaging for the diagnosis.
1. Clinical manifestations
The clinical manifestations of LM are varied, depending on the site of tumor cell invasion, and can produce multifocal signs and symptoms or isolated neurological involvement.
LM usually presents with parenchymal brain involvement and symptoms of meningeal irritation (including headache, dizziness, nausea, vomiting, neck stiffness, difficulty walking, altered mental status, seizures, and impairment of consciousness, cognition, and sensation, with headache being the most common), cranial nerve involvement, and spinal cord and spinal nerve root irritation.
So, patients with NSCLC who develop these symptoms need to seek prompt medical attention and be alert for the presence of meningeal metastases.
2. Imaging examinations
Contrast-enhanced MRI of the whole brain and whole spinal cord with gadolinium is the most valuable imaging test for the diagnosis of LM, with a sensitivity of 70-85% and specificity of 75-90% for the diagnosis of solid LM tumors. For patients with NSCLC with typical clinical symptoms, the typical presentation of enhanced MRI can be used as a diagnostic basis for LM for physicians’ reference.
It is important to note that 20% to 30% of patients who undergo a lumbar puncture followed by an enhanced MRI will have a false-negative result, so physicians often perform an enhanced MRI before performing a lumbar puncture to avoid this.
3. Cerebrospinal fluid (CSF) examination
(1) CSF cytology
CSF cytology tests to find tumor cells are the gold standard for the diagnosis of LM. However, the sensitivity of a single lumbar puncture is only 50%, so usually physicians recommend that patients undergo 2 lumbar punctures, which can increase the sensitivity to 75%-85%, and the diagnostic benefit of 3 or more lumbar punctures is minimal, so there is no need to perform multiple lumbar punctures to improve detection rates.
In addition to cytology, novel assays have been helpful in the diagnosis of LM, and new technologies such as immunofluorescent staining for CSF tumor markers with chromosomal fluorescence in situ hybridization (TM-iFISH), CSF circulating tumor cell detection (CTC), and cellsearch have been used to partially improve detection rates.
(2) Tumor marker assays
Tumor markers commonly used clinically for CSF detection include CEA, NSE, and Cyfra21-1, and their elevation is suggestive for the diagnosis of LM.
(3) Gene mutation testing
Liquid biopsy is a new technique for tumor diagnosis in recent years, and the accuracy of ctDNA in cerebrospinal fluid is much higher compared with peripheral blood circulating tumor DNA (ctDNA). In other words, the use of liquid biopsy techniques to diagnose LM is now of high value. The CSF test mentioned above also happens to be a source of specimens for EGFR, ALK, and other genetic tests.
Notably, the genetic alterations in LM metastases may be different from the primary and remaining metastases, and current studies suggest that EGFR T790M mutations are detected less frequently in LM metastases than in extracranial specimens, whereas MET amplification is more frequent in cerebrospinal fluid than EGFR T790M mutations.
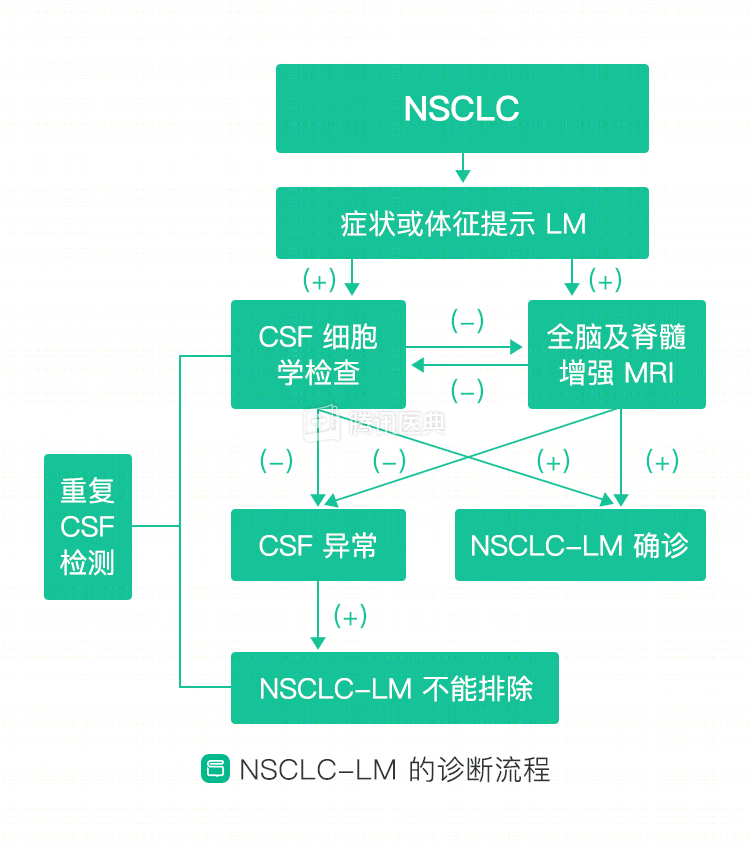
4. LM diagnostic process
After describing the diagnostic approach described above, let’s look at the specific process that physicians use to diagnose NSCLC-LM according to the US NCCN guidelines (Figure).