
There are three main ways to screen for breast cancer that are most commonly used and effective:
- Examinations, where an experienced physician can screen a subset of patients by performing a breast exam;
- Ultrasound, which can determine possible abnormalities in the breast by changes in the breast structure and blood supply;
- X-ray, which can determine the likelihood of early breast cancer by a number of signs.
Other methods other than these, such as the following three, are not recommended by doctors for breast cancer screening.
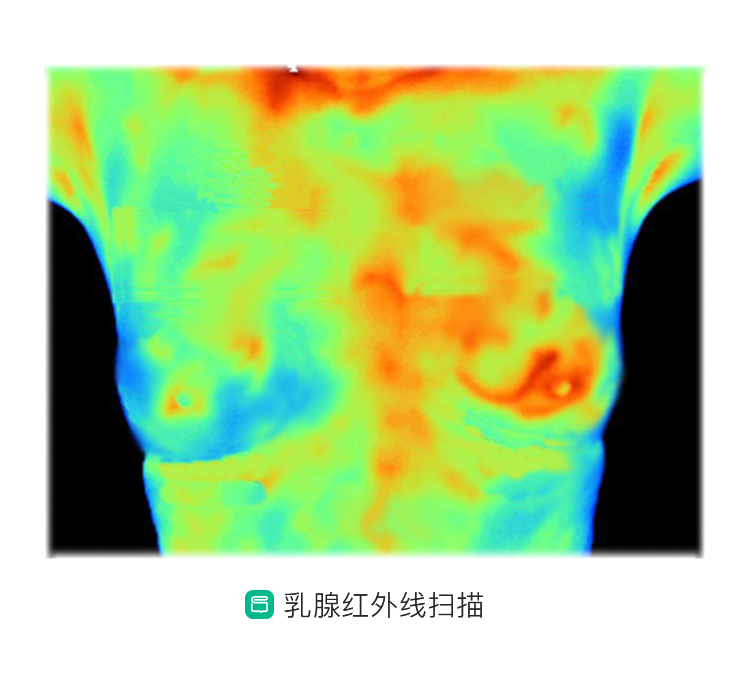
Infrared scan of the breast
Breast infrared scans use an infrared probe to transmit light to the breast tissue and image it according to the body’s principle that tissue absorbs infrared light differently. Usually the doctor will determine the presence of a lesion based on the depth of the shadow and identify the benignity or malignancy of the swelling based on the borders of the swelling and the distribution of blood vessels (i.e., heat around the swelling).
As the name implies, transillumination is a light-transmitting principle, and the shadow can only be seen if the mass grows to a certain size. Therefore, breast infrared scans are highly likely to miss the diagnosis of small masses or breast disease without a mass. Due to the different degrees of infrared heat sensitivity, the peripheral heat can vary even for the same mass at different times or when detected by different people. Therefore, determining the benign or malignant nature of a mass on this basis is highly influenced by individual subjectivity, and the accuracy of the results is highly variable.
Breast nuclide scan
Radionuclide scanning is the use of imaging instruments to obtain images of organs or lesions based on the difference in uptake of the radiopharmaceutical between the inside and outside of the organ or between normal tissue and the lesion after the radiopharmaceutical is introduced into the body. The resolution of this method is inferior to other imaging detection methods, the clarity is poor, and the sensitivity is significantly lower for malignant tumors smaller than 1 cm.
In breast nuclide scans, the ability of different types of breast cancer tumor cells to take up radiopharmaceuticals and the rate of uptake vary greatly, and the abundance of cancer cells, the amount of blood supply, and the presence or absence of necrosis can affect the concentration of nuclide and thus the results. (no breast cancer but diagnosed as breast cancer). These uncertainties and inaccuracies greatly limit its use in early breast cancer screening.
Breast oxygen functional imaging
Tumor growth is dependent on abundant neovascularization around the tumor, while local necrosis of cancerous tissue, poor circulation, and high metabolism of cancer cells can all contribute to reduced blood oxygen levels inside the tumor. Therefore, malignant tumors are characterized by high external blood flow and low internal blood oxygenation. The results of this study are summarized below.
The test is based on an infrared scan of the breast, which has an inevitably low sensitivity and high error rate, as well as structural differences in breast parenchyma, differences in the local sensitivity of the light source to the breast, and internal heterogeneity of the tumor, which can significantly affect the accuracy of the local oxygenation of the tumor.
In conclusion, the above three tests are not currently recommended for early screening of breast cancer because of their respective disadvantages. The primary and effective imaging methods for clinical breast cancer screening are still ultrasound and mammography, sometimes in combination with each other. In addition, if further confirmation is needed, breast magnetic resonance imaging (MRI) is also an ideal option.