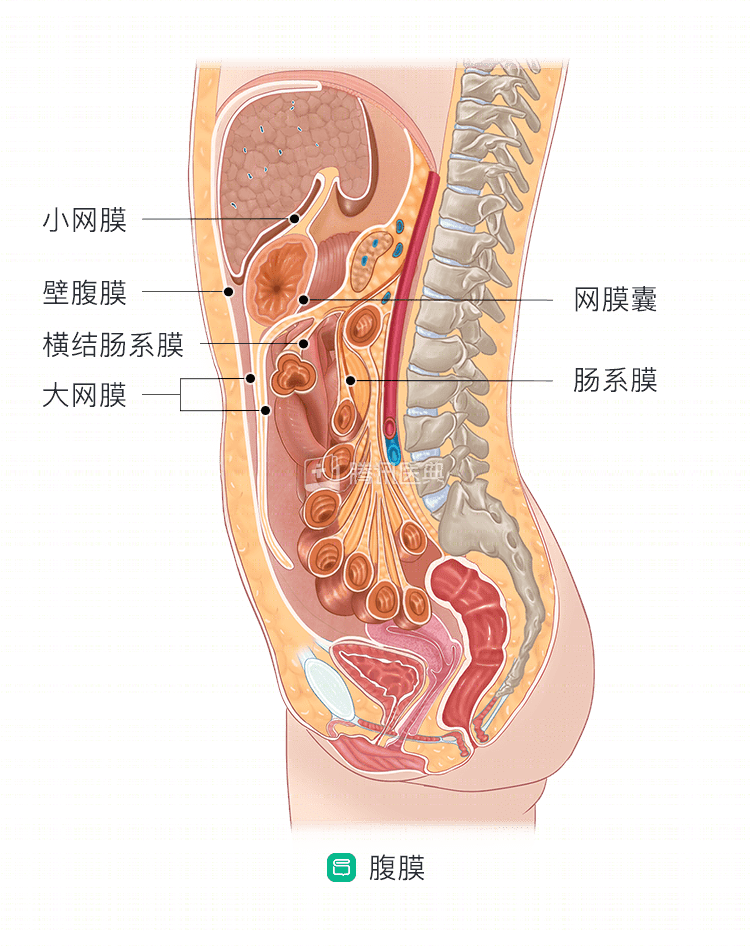
The peritoneum is a thin, smooth plasma membrane that covers the walls of the abdominal and pelvic cavities (called the mural peritoneum) and the surfaces of the abdominal and pelvic organs (called the visceral peritoneum), which together enclose an irregular underlying cavity called the peritoneal cavity. The cavity contains only a small amount of plasma that has a lubricating effect, and in lesions can produce a large volume of fluid, called ascites.
The peritoneum migrates back and forth, longitudinally and horizontally, between the abdominal organs, forming the greater omentum, lesser omentum, tethering, ligaments, and many other structures (as shown), which serve to connect and anchor organs, and also serve as a pathway for blood vessels, nerves, and other access to organs
Looking again at the esophagus, its microscopic structure consists of 4 layers, namely the mucosa, submucosa, muscularis, and epithelium. When the cancer cells penetrate the muscular layer of the esophagus, they are easily shed outside the esophagus. The peritoneum is one of the possible “destinations” for the cancer cells.
Does esophageal cancer develop peritoneal metastases?
Esophageal cancer is less likely to metastasize peritoneally. Those that do tend to metastasize to the peritoneum are usually adenocarcinomas. The mechanism of metastasis is similar to that of gastric cancer, i.e. cancer cells that leave the primary site grow directly via bloodstream, lymph or peritoneum to form metastases. The occurrence of peritoneal metastasis depends on the microenvironment of cancer cells (seeds) and the peritoneum (soil). When the seeds encounter the right soil, they colonize and keep proliferating into tumors.
What are the manifestations of peritoneal metastasis? How is it diagnosed?
Peritoneal metastases can cause many different symptoms, including abdominal distention, decreased food intake, and impaired bowel elimination; in severe cases, they can cause intestinal obstruction; rupture of the metastases can cause abdominal bleeding; and as the metastases progress, they often produce ascites.
To confirm the diagnosis of peritoneal metastasis, the physician needs to take a detailed history, perform a physical examination, and rationalize hematologic laboratory tests, imaging tests, and, if necessary, pathologic biopsy for diagnosis.
Is it still possible to treat peritoneal metastases after they occur?
The treatment of peritoneal metastases from esophageal cancer includes, palliative chemotherapy, peritoneal perfusion chemotherapy and peritoneal thermal perfusion chemotherapy, and palliative surgery, which requires a multidisciplinary and comprehensive approach.
- Systemic systemic chemotherapy is the cornerstone of treatment of peritoneal metastases from esophageal cancer. Peritoneal infusion chemotherapy as a complementary treatment can improve local drug concentration and reduce systemic adverse effects.
- Palliative surgery may be considered for symptomatic relief in the presence of surgical emergencies, such as intestinal obstruction, bleeding, and intractable ascites.
- Aggressive symptomatic supportive treatment and psychological relief therapy are important to improve the overall quality of life.