Once a doctor determines a patient’s prostate cancer stage, he or she can begin to develop a treatment plan in conjunction with his or her physical condition. Prostate cancer staging depends on:
- the size of the primary tumor;
- Lymph node metastasis;
- Distant metastases (bone, visceral metastases, etc.).
There is no strict corresponding treatment plan for different stages of prostate cancer, and the decision of which treatment plan to choose needs to be made by both the patient and the doctor.
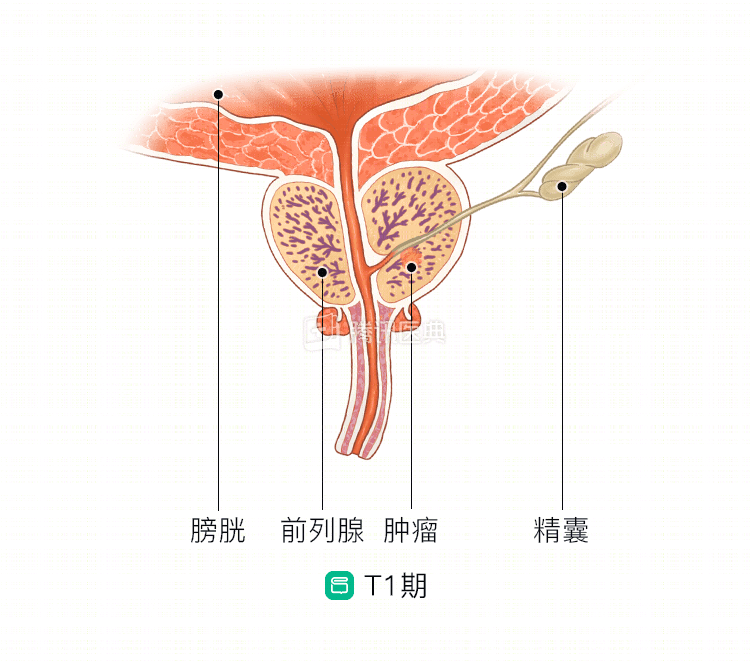
Stage I
The tumor is small, confined to the prostate, and the cancer cells grow slowly and may never cause symptoms or other health problems.
Patients usually have low prostate-specific antigen (PSA) levels and Gleason scores, suggesting that they are doing well. However, when PSA and Gleason scores are high, the cancer is more aggressive and more likely to recur, metastasize, and require intensive treatment.
The PSA test examines the amount of prostate-specific antigen (a protein) in the blood, and the Gleason score is determined by a pathologist based on the morphology of prostate tissue cells viewed under a microscope.
Patients with stage I prostate cancer should consider the following treatment modalities:
- Active surveillance: PSA levels are tested regularly. If PSA levels are elevated, it may mean that the tumor is growing or the cancer has a tendency to spread, and further testing and treatment is needed.
- Watch and wait: Watch and wait requires fewer tests than active surveillance, but requires close attention to your symptoms. Doctors often recommend watchful waiting if the patient is older, has other serious medical conditions, or if the patient is unwilling to accept other options.
- Radiotherapy: This kills prostate cancer cells, thus stopping them from growing and dividing further. There are two types of radiation therapy: external radiation therapy, which uses a machine to focus radiation on the tumor; and internal radiation therapy, which involves implanting radioactive particles inside the tumor or next to the cancer – a process also known as brachytherapy.
- Radical prostatectomy: This is the surgical removal of the prostate and surrounding tissue.
- Ablation therapy: Uses freezing or high-intensity ultrasound to kill cancer cells.
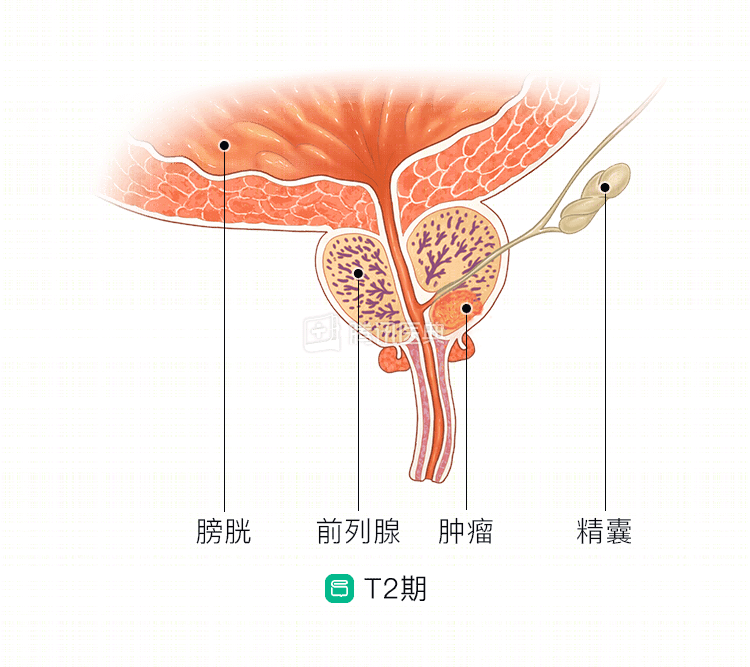
Stage II
This is when the tumor is large but confined to the prostate and has not spread outward, and PSA levels and Gleason scores are high. stage II includes both stage IIA and stage IIB. Surgery or radiation therapy is usually necessary to prevent the cancer from spreading.
Patients with stage II prostate cancer may consider the following treatments:
- Active surveillance: Active surveillance is often an option if the patient is older or in poorer health.
- Radiotherapy: This can be combined with endocrine therapy as co-treatment. Endocrine therapy reduces the production of androgens, which inhibits the growth of cancer cells.
- Radical prostatectomy.
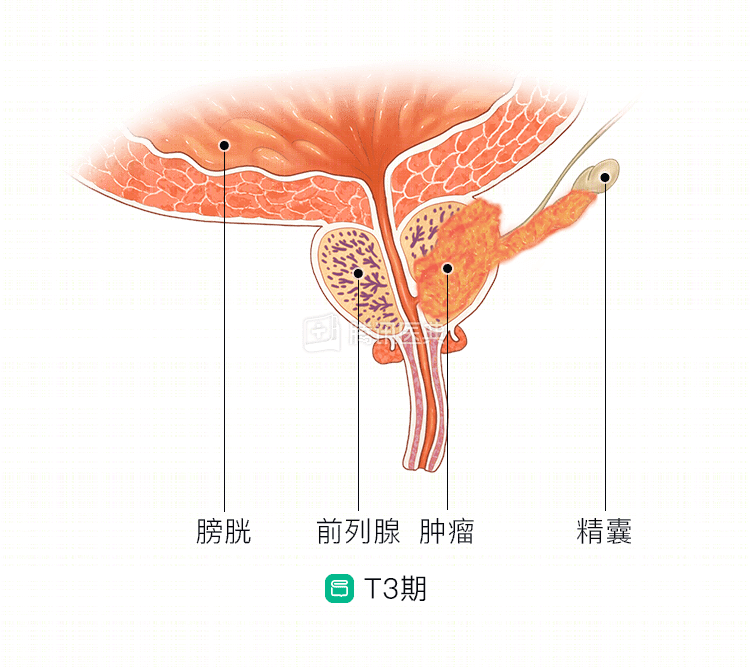
Stage III
At this point, the cancer has spread beyond the prostate, but has not yet spread to the bladder, rectum, lymph node groups, and adjacent organs.
Patients with stage III prostate cancer may consider the following treatments:
- External radiotherapy combined with endocrine therapy.
- External radiotherapy and internal radiotherapy combined with endocrine therapy.
- Radical prostatectomy, often combined with pelvic lymph node dissection. The surgeon may recommend postoperative radiotherapy or endocrine therapy, and sometimes preoperative endocrine therapy may be recommended.
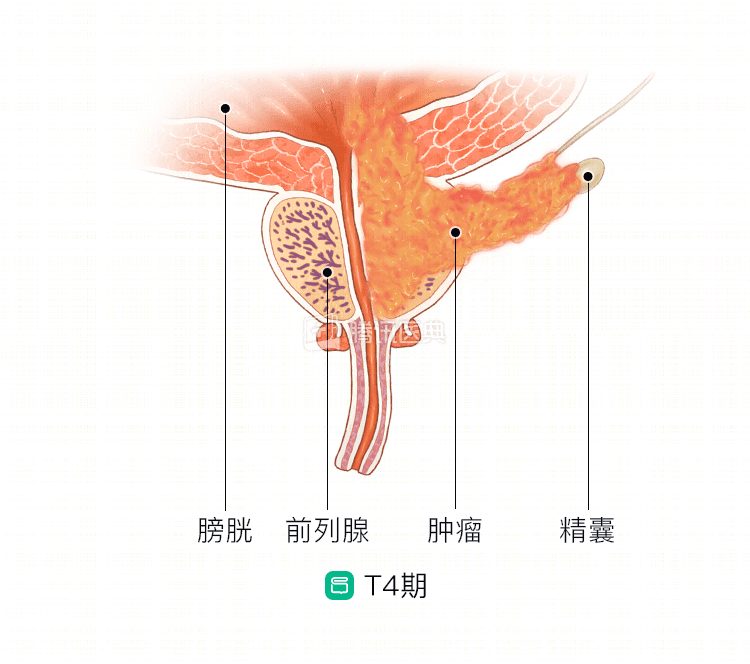
Stage IV
This is when the cancer has spread to the bladder, rectum, lymph nodes, other organs, or bones. Stage IV patients are largely incurable, but treatment can reduce pain and improve survival.
Stage IV prostate cancer patients may consider the following treatments:
- Endocrine therapy: Usually combined with surgery, radiation or chemotherapy.
- Endocrine therapy: usually combined with surgery, radiation or chemotherapy.
- Surgery: Relieves symptoms such as bleeding or urinary tract obstruction and removes lymph nodes that have metastasized prostate cancer cells.
- External radiation therapy: Sometimes combined with adjuvant endocrine therapy.
- Chemotherapy: If standard treatment fails to relieve symptoms and the cancer continues to grow, chemotherapy may be given to reduce the size of the tumor and slow the growth of the cancer cells.
- Biphosphonates: Help slow the growth of cancer cells in the bones and prevent pathological fractures.
- Sipuleucel-T vaccine: Helps activate the immune system so that cancer cells are recognized and killed. It may be considered when endocrine therapies do not work.
- Palliative care: Designed to relieve patients of symptoms such as pain and difficulty urinating.
Also, patients can ask their doctor if there is an appropriate clinical trial.
Recurrence of prostate cancer
If the cancer recurs after remission is achieved, then subsequent treatment depends largely on the site of the cancer and previous treatment.
Prostatectomy may be an option if the tumor is confined to the interior of the prostate; radiotherapy may be an option if a radical prostatectomy has been received; radical prostatectomy may be an option if radiotherapy has been received; and cryosurgery may also be considered.
If the tumor has metastasized and spread to other parts of the body, endocrine therapy may be the most effective treatment option. External radiation therapy for ≤3 metastases may prolong survival, and intravenous bisphosphonates may relieve bone pain from bone metastases and prevent pathologic fractures.
Related reading: