What is Macroscopic Liver Cancer?
The classification of hepatocellular carcinoma was established in 1901 by Eggel.
Eggel’s classification of hepatocellular carcinoma into giant, nodular, and diffuse types in 1901 has been used to date. subclinical hepatocellular carcinoma or small hepatocellular carcinoma was identified in the 1970s due to the use of serologic tumor markers for screening. In response, the Domestic Hepatology Collaborative Group on Hepatocellular Carcinoma was divided into
on the basis of Eggel’s classification.
- Mass type, i.e., single mass, fusion mass, and multiple masses
- Nodular type, i.e., single nodule, fused nodule, multiple nodules
- Diffuse type
- Small carcinoma type
This classification of giant hepatocellular carcinoma is therefore used less frequently and is currently classified as massive, nodular, diffuse, and small carcinoma.
How is giant hepatocellular carcinoma treated?
Before treatment, liver cancer needs to be staged.
There are various staging options abroad, such as BCLC, TNM, JSH, APASL, and so on. The following stages of liver cancer are recommended in the 2017 edition of the Standardized Practice for the Treatment of Primary Liver Cancer in China: stage Ia, stage Ib, stage IIa, stage IIb, stage IIIa, stage IIIb, and stage IV. The specific staging and treatment options are shown in the figure:
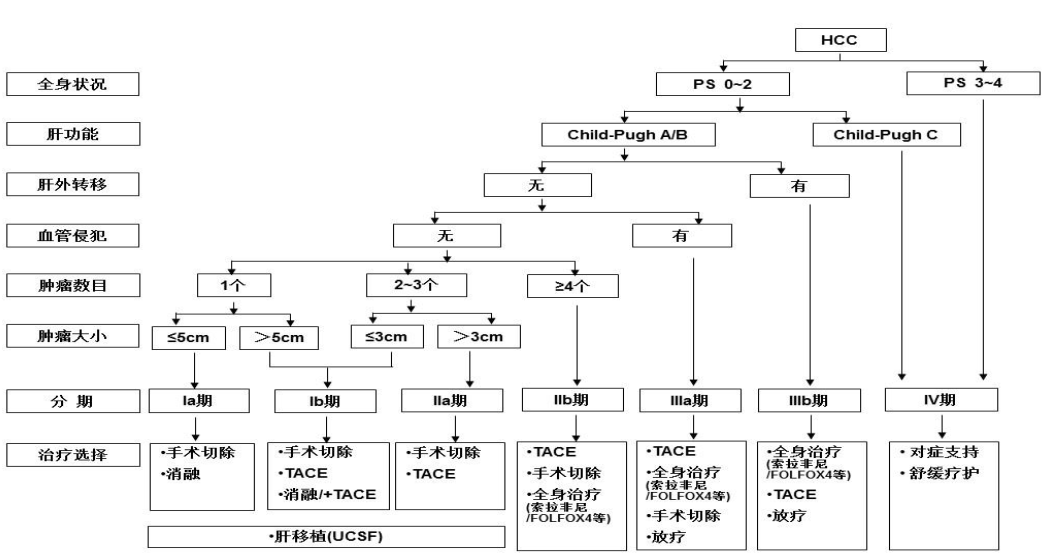
The “jargon” of the above treatment plan is a bit difficult to understand, so I will “translate” it for you.
HCC
HCC
Hepatocellular carcinoma (HCC) is the most common type of chronic liver cancer in adults and the most common cause of death in patients with cirrhosis.
Child-Pugh rating of liver function
A clinically common grading scale for quantitative assessment of liver function is based on three levels of patient status across five indicators, including hepatic encephalopathy, ascites, serum bilirubin, serum albumin concentration, and prothrombin time.
A score of 1, 2, and 3 was recorded, and the 5 index scores were summed, with a minimum sum score of 5 and a maximum score of 15, thus classifying liver function into A, B, and C levels according to the magnitude of this sum, predicting three different levels of severity of liver damage (the higher the score, the worse the liver reserve function).
Physical activity status PS score
Physical activity status (PS) is an index used to understand their general health status and ability to tolerate treatment.
Ablation
A probe or needle is inserted into a tumor under CT or MRI guidance and uses heat from an electric current, or ultra-low temperature from a cryogen, such as argon, to “scald” or “freeze” the tumor to death.
For hepatocellular carcinoma less than 3 cm in diameter, this is a very effective treatment. For hepatocellular carcinoma larger than this size, ablation can be used in combination with interventional therapy.
TACE
After selective insertion of a catheter into the target tumor-supplying artery, the right amount of embolic drug is injected at the right rate to occlude the target artery and cause ischemic necrosis of the tumor tissue, called transcatheter arterial chemoembolization (TACE).
Radiotherapy
The guidelines recommend radiotherapy, including stereotactic radiotherapy, intensity-modulated conformal radiotherapy, and 3-dimensional conformal radiotherapy. Among them, stereotactic radiotherapy can focus more precisely on the cancer and deliver a higher single dose, which is like an invisible “radiographic knife” that cuts the tumor cleanly, mainly for patients with three or fewer tumors.
The intensity-modulated conformal radiotherapy and 3D conformal radiotherapy can adapt to the shape of the tumor and deliver radiation to the tumor from many different angles to achieve the best treatment effect.
Symptomatic supportive and palliative therapies
Specific treatment includes analgesia, correction of anemia, correction of hypoproteinemia, and nutritional support therapy. For patients with complications such as ascites, jaundice, hepatic encephalopathy, gastrointestinal bleeding, and hepatorenal syndrome, the guidelines recommend symptomatic management to reduce patient distress.
The field of hepatocellular carcinoma treatment is characterized by the coexistence of multiple approaches such as surgical resection, liver transplantation, ablation, TACE, targeted therapy, radiotherapy, and immunotherapy, and the collaboration of multiple disciplines such as hepatobiliary surgery, medical oncology, and interventional therapy, so that hepatocellular carcinoma treatment is currently a multidisciplinary team model that requires problem-specific analysis.