Before answering questions related to bone metastases from esophageal cancer, let’s get to know our bones.
Bones are highly dynamic organs that undergo constant change and regeneration.
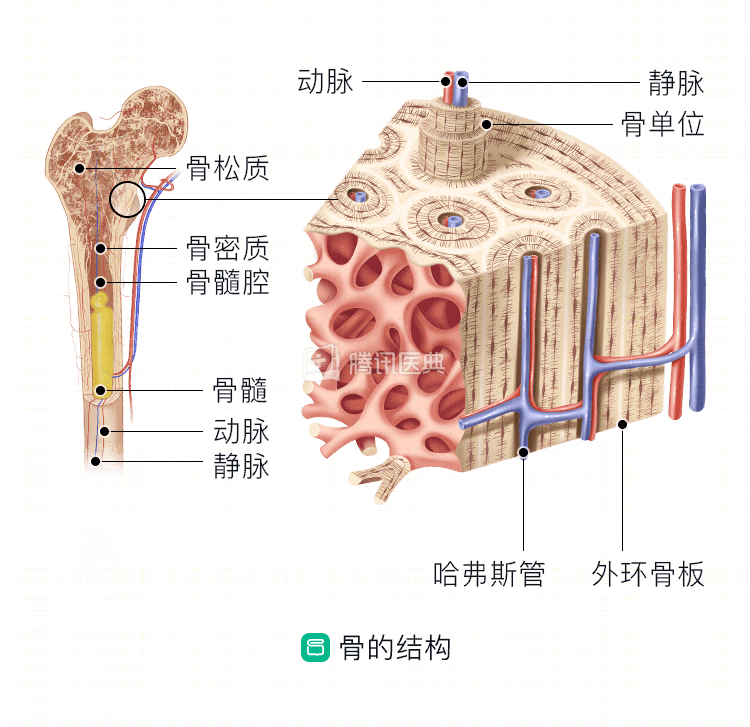
The remodeling process of normal bone involves resorption of bone by osteoblasts and deposition of new bone by osteoclasts. Bone consists of specialized osteocytes, mineralized and nonmineralized connective tissue matrix, and voids (voids include marrow cavities, vascular channels, bone tubules, and traps containing osteocytes). The structure of bone is shown in the following two figures:
Why does esophageal cancer develop bone metastases? Which bones are prone to metastasis?
Bone metastasis is less common in esophageal cancer. The most common route of metastasis is hematogenous, where the cancer cells are like seeds that travel throughout the body with the blood flow and settle in the right soil to proliferate into tumors.
Bone metastases are usually divided into two categories: osteolytic bone metastases, which are characterized by destruction of normal bone, and osteogenic bone metastases, which are accompanied by new bone deposition, and are distinguished mainly by radiographic manifestations. Bone metastases from esophageal cancer can have both osteolytic and osteogenic lesions.
The human skeleton can be divided into mesial bones (consisting of the skull, spine, sternum, and ribs) and limb bones. Bone metastases from esophageal cancer most often occur in the spine, followed by the pelvis and ribs, and sternal metastases are relatively uncommon.
What are the symptoms of bone metastasis? How do doctors diagnose them?
Bone metastases from esophageal cancer can cause many different symptoms, with immediate complications including severe pain, pathological fractures, and epidural spinal cord compression, and osteolytic bone metastases can lead to life-threatening hypercalcemia.
To confirm the diagnosis of bone metastases, physicians need to take a detailed history, perform a physical examination, and rationalize hematologic tests, imaging, and, if necessary, pathologic biopsy.
- For symptoms and physical examination, the doctor will pay attention to whether you have pain, low back pain, numbness in the limbs, paraplegia, and limited spinal movement;
- For hematology tests, the doctor will usually prescribe serum calcium tests, renal function tests, and serum alkaline phosphatase tests.
- Imaging methods used to assess the morphology and function of bone metastases include X-ray, CT, MRI, bone imaging (BS), SPECT/CT (single photon emission computed tomography), and PET/CT. A reasonable mix of different imaging modalities can improve the detection rate of bone metastases.
- X-rays and CT can better show the extent of bone destruction;
- MRI is the best test to evaluate the bone marrow and detects early intramedullary malignant lesions, but MRI is not as sensitive as CT for cortical lesions;
- Bone scan shows the whole body skeleton and is the imaging test of choice for patients with high-risk bone metastases.
- PET (positron emission tomography) is a functional imaging modality that can detect functional changes in bone and bone marrow caused by tumor bone metastases before morphologic changes in the bone marrow.
- If the diagnosis is doubtful, pathologic biopsy of the lesion is required if necessary, and pathologic diagnosis is the gold standard for all tumor diagnoses.
Is bone metastasis from esophageal cancer still treatable?
The treatment of esophageal cancer after bone metastasis includes palliative radiotherapy, chemotherapy, and surgery, and requires comprehensive treatment with multidisciplinary collaboration, aiming to reduce pain, prevent fractures, and improve quality of life.
Bone pain is the most prominent symptom. Osteoclasts are a major influence in cancerous bone pain and release protons that cause bone pain (protons activate the acid sensory receptor TRPV1, expressed on sensory neurons in bone, to induce pain). Osteoclast inhibitors such as bisphosphonates and denosumab are effective in reducing bone pain.
Local palliative radiotherapy is fast-acting and effective in relieving bone pain. Palliative radiotherapy of weight-bearing bones (e.g., femur, tibia) is effective in preventing pathologic fractures. If a fracture occurs in a weight-bearing bone, surgery can improve the patient’s mobility and quality of life.
Aggressive symptomatic support and psychological support treatment are both important to improve the overall quality of life of patients.