Before answering the questions related to lung metastases from esophageal cancer, let’s get to know our lungs.
The lungs are important respiratory organs of the body, located in the thoracic cavity, one on each side. The two lungs are separated by a mediastinum composed of the heart, trachea, esophagus, blood vessels, and other tissues and organs, so they are relatively independent.
The lung tissue can be divided into parenchyma and interstitium. The parenchyma is the bronchial branches of the lungs and the large number of alveoli at their termini; the interstitium includes the connective tissue of the lungs and the blood vessels, lymphatics, and nerves within it.
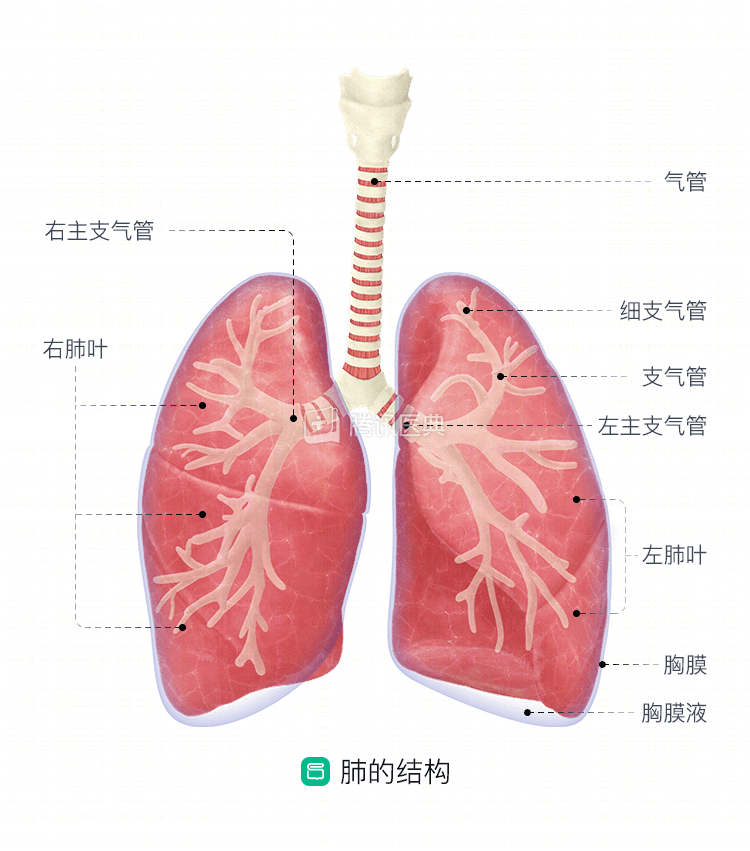
There are two sources of blood supply to the lungs, the pulmonary arteries and the bronchial arteries. The pulmonary artery is a functional vessel that emanates from the right ventricle and enters the lung at the pulmonary hilum, and its branches travel with the bronchi at all levels up to the alveolar septum, forming a capillary network where blood exchanges gases with the alveoli, and then returns to the left heart via all levels of veins into the pulmonary veins, supplying the oxygen needs of the whole body with the body circulation. The bronchial arteries are the nutrient vessels of the lungs, originating from the thoracic aorta or intercostal arteries, and are used to nourish the tissues within the lungs. The general structure and organization of the lungs are shown in the figure below.
The lung is a more frequent organ for distant metastases from esophageal cancer, second only to the liver.
The most common mechanism of pulmonary metastasis is hematogenous dissemination. Because venous blood flowing out of the esophagus eventually returns to the right heart, it then travels through the pulmonary circulation to the intrapulmonary capillary bed, which is narrow in diameter and therefore tumor masses tend to be retained. The localization and growth of cancer cells within the lung is determined by a combination of its own characteristics and certain factors within the lung microenvironment. To form metastases, cancer cells need not only to have a strong tumorigenic capacity in themselves, but also to have the ability to evade immune surveillance and killing by immune cells within the local lung microenvironment.
The relationship is like that between seeds and soil, where the seeds need to have a strong capacity to grow and the soil needs to provide the right environment for the seed to grow into a plant. In tumor lung metastasis, the cancer cells are the seeds and the lung microenvironment is the soil.
What are the symptoms of lung metastasis? Can I catch it early?
Pulmonary metastases can cause many different symptoms, including irritating dry cough, coughing up sputum (metastases invading blood vessels can result in blood in the sputum or even hemoptysis), chest pain (significant chest pain when metastases invade the pleura), and difficulty breathing.
These symptoms are not unique to tumors, and many benign diseases can have similar symptoms, so a differential diagnosis by a medical professional is needed.
How do doctors confirm the diagnosis of lung metastases?
To confirm the diagnosis of pulmonary metastases, physicians need to take a detailed history, perform a physical examination, and arrange reasonable hematologic tests, imaging, and, if necessary, a pathologic biopsy for diagnosis.
- For symptoms, attention needs to be paid to the presence of cough, coughing sputum, chest pain, hemoptysis, fever, etc.
- For physical examination, the presence of hypopnea or abnormal breath sounds, and the presence of hypoxic manifestations are needed.
- Chest X-ray or CT can detect intrapulmonary occupancies, and PET/CT can perform functional imaging of systemic lesions, which is more helpful in identifying benign and malignant lesions.
- If the diagnosis is doubtful, puncture biopsy can be performed if necessary, and pathological diagnosis is the gold standard.
.
With lung metastases, can they still be treated?
The treatment of esophageal cancer after lung metastasis occurs, including palliative surgery, palliative radiotherapy, and local interventions, requires comprehensive treatment with multidisciplinary collaboration.
- For cases with more limited metastases, surgical resection can be considered.
- For lesions that are difficult to remove surgically, local radiotherapy and radiofrequency ablation can be attempted to destroy the lesion.
- Palliative chemotherapy can control both primary and metastatic lesions, and the patient’s tolerance and tumor sensitivity to the drug need to be considered to choose the treatment plan.
- Local interventions such as embolization of tumor-supplying arteries may also play an important role in controlling the progression of pulmonary metastases and in treating life-threatening complications such as tumor rupture and bleeding.
- Aggressive symptomatic supportive therapy and psychological support therapy are important in improving the overall quality of life.