Compared to surgical open-heart or thoracoscopic surgery, endoscopic resection is easy to perform, less invasive, with fewer complications and shorter operative time and hospital days, and patients recover quickly and have a better quality of life after surgery .
However, not all patients with esophageal cancer are suitable for endoscopic resection.
Am I a candidate for endoscopic resection?
Esophageal cancer is divided into squamous and adenocarcinoma, and the vast majority of our patients have squamous cancer, so this article focuses on patients with squamous cancer.
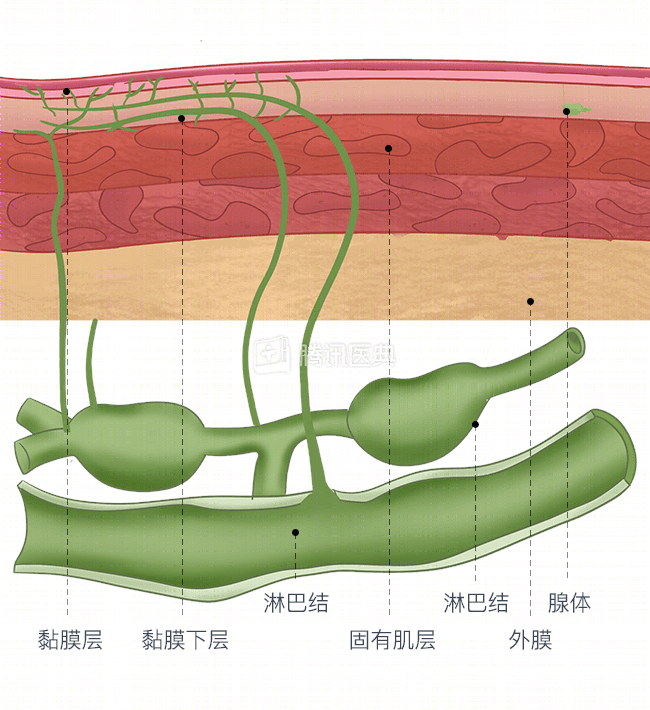
The earlier the stage of squamous esophageal cancer, the less likely the cancer is to metastasize to the lymph nodes and the better the treatment outcome. The endoscopic resection can only destroy the primary site, but not the metastases that have “escaped” to the mediastinal lymph nodes.
It is like a watermelon, where the rind is the mucosa (the most superficial layer of tissue in the esophagus) and the seeds are the lymph nodes. If only the rind of the watermelon is rotten, cut it off and this watermelon is still good. But when the flesh of the watermelon is also rotten, the risk of the watermelon seeds rotting is high, and then just cutting off the rind of the watermelon is not enough.
So, endoscopic resection is indicated for early-stage cancer that invades only the mucosal layer (see below) and excludes lymph nodes and metastases to other organs.
How can I tell if it is early stage cancer and if there are lymph node metastases?
Gastroscopy, ultrasound gastroscopy, and enhanced CT chest examination can determine the early and late stages of esophageal cancer and lymph node metastasis.
For patients with suspected esophageal cancer, gastroscopy provides a comprehensive screening of the upper gastrointestinal tract (including the oropharynx, esophagus, stomach, and duodenum) to visually identify tumor lesions. Doctors can also remove biopsies for pathological examination under gastroscopy to clarify whether it is esophageal cancer and to stage it.
If early-stage esophageal cancer is initially suspected after gastroscopy, magnified gastroscopy, ultrasound gastroscopy (EUS) and enhanced CT of the chest are also needed to clarify the depth of tumor invasion, the presence of lymph node metastasis, etc.
Amplifying gastroscopy has a zooming front end that allows magnification of the suspected lesion and facilitates observation of fine structures, which helps to detect microscopic lesions and determine the depth of cancer infiltration. The ultrasound endoscope places a miniature high-frequency ultrasound probe at the front end, which allows both direct observation of tissue patterns in the esophageal lumen and real-time ultrasound scanning, showing the structural layers of the esophageal wall layer by layer to determine which layer the cancer has invaded and to understand the metastasis of surrounding lymph nodes.
Plain CT scan can show the thickness of the esophageal wall, the extent of tumor infiltration, the degree of involvement of surrounding tissues, and whether metastasis has occurred; enhanced CT with water-soluble organic iodine injection makes the image of the aorta more visible and clearly separated from the esophagus, reducing the probability of false positives and reducing the number of “false positives” and avoiding overtreatment. The result is that the probability of false positives is greatly reduced, reducing “false positives” and avoiding overtreatment.
To understand the procedure of endoscopic resection, please read: