For patients with resectable esophageal cancer, surgery is the most important and central treatment, and the only one that is likely to achieve a curative effect. However, it is also important for you to understand that surgery, while important, is not the entirety of esophageal cancer treatment. Before surgery, your doctor will need to complete the relevant evaluation, perform the necessary preoperative neoadjuvant therapy, supportive therapy during surgery, and postoperative adjuvant therapy and follow-up.
But there are some cases where surgery does not result in a “radical” resection. Why is this the case? Can this be remedied? Here is a real-life case study to explain.
Case presentation
Mr. Ma, 59 years old, presented with dysphagia for more than 6 months and underwent gastroscopy and PET-CT after consultation, which revealed an elevated lesion 26 cm from the incisor and an irregular mass at 30 cm from the incisor, with pathologic biopsy suggesting a high-grade differentiated squamous carcinoma; the lower and middle esophageal segments and the upper The tumor may have invaded the lumen of the middle and lower esophagus, and there are enlarged lymph nodes in the mediastinum, with no clear signs of distant metastasis in other parts of the body.
The final diagnosis was: multiplc primary esophageal carcinoma (MPEC), with clinical stage III.
Course of treatment
According to the National Comprehensive Cancer Network (NCCN) guidelines, Mr. Ma was given preoperative “neoadjuvant chemotherapy” with “paclitaxel + cisplatin”. The post-chemotherapy review showed that the tumor had shrunk slightly from the previous size (below), and the dysphagia symptoms had subsided. 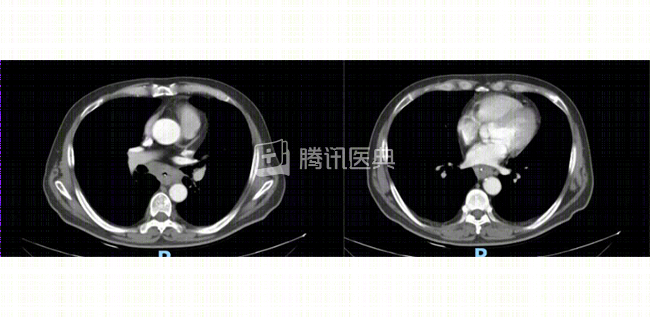 Note: Pre-chemotherapy chest CT suggested that the wall of the lower thoracic segment of the esophagus was significantly thickened with enlarged mediastinal lymph nodes, and the border between the tumor and the lower pulmonary vein was blurred
Note: Pre-chemotherapy chest CT suggested that the wall of the lower thoracic segment of the esophagus was significantly thickened with enlarged mediastinal lymph nodes, and the border between the tumor and the lower pulmonary vein was blurred
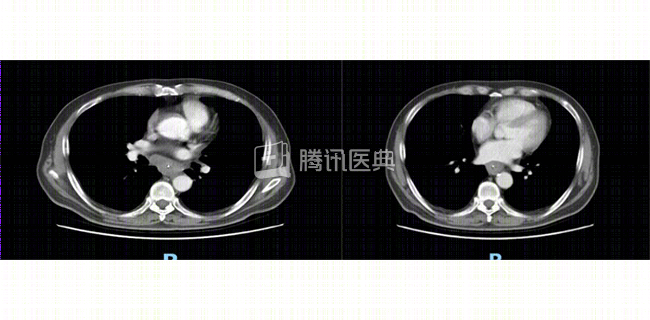 Note: The CT was repeated after chemotherapy. The lymph nodes were still enlarged and the tumor was still closely related to the inferior pulmonary vein
Note: The CT was repeated after chemotherapy. The lymph nodes were still enlarged and the tumor was still closely related to the inferior pulmonary vein
He was treated with follow-up surgery. The tumor was found to have invaded the lower pulmonary vein and could not be removed in its entirety, but had to be removed palliatively.
Postoperatively, Mr. Ma recovered well and received additional radiation therapy targeting the tumor bed and mediastinal lymph nodes.
A review about 5 months after surgery revealed multiple metastases throughout the body. Although aggressive symptomatic treatment was given immediately, it still did not save his life.
Summary
After reading Mr. Ma’s case, you may have many questions, which we will answer below.
Question 1
What did the doctor consider when choosing the preoperative neoadjuvant therapy + postoperative adjuvant radiotherapy regimen?
The doctor said:
The first thing to understand is that the preoperative workup for esophageal cancer includes two aspects:
- Examinations to assess tumor staging, including: gastroscopy, ultrasound gastroscopy, chest-enhanced CT, upper gastrointestinal imaging, and whole-body PET-CT.
- Examinations to assess physical condition to tolerate surgery, including: electrocardiogram, cardiac ultrasound, pulmonary function tests, etc.
Mr. Ma’s preoperative staging suggested locally advanced disease with no clear signs of distant metastases systemically, and his cardiopulmonary function was assessed to be able to tolerate surgery. According to authoritative NCCN guidelines, this case should be treated with preoperative neoadjuvant therapy first, and if the tumor shrinks and clinical symptoms resolve after treatment, the surgeon can proceed with further surgery.
Question 2
What is a “palliative” resection?
Doctors say:
The degree of radicality of surgical resection is divided into: R0, R1, and R2.
R0 resection means that the tumor is completely removed, i.e., “radical resection”;
R0 resection means that the tumor is completely removed, i.e., “radical resection”;
R1 resection means that the tumor was visually determined to be complete, but postoperative pathology suggests residual tumor;
R2 resection means that there is intraoperative tumor residual as determined by the naked eye.
In Mr. Ma’s case, intraoperative exploration revealed that the tumor showed extranodal growth and invaded the inferior pulmonary vein, which could not be completely freed. The tumor was found to be invasive and invaded the inferior pulmonary vein, which is the “pathway” for the return of venous blood to the heart, and any damage would be unacceptable. Therefore, the tumor cannot be completely removed, but can only be palliatively removed, which is medically known as “R2 resection”. This means that the residual tumor will “come back” in a short period of time.
Question 3
Why didn’t Mr. Ma get a radical resection?
Doctors say:
The ability to get a radical resection can be determined somewhat based on preoperative imaging. If the tumor is found to have no clear boundary with the surrounding tissues, the possibility of invasion of surrounding organ tissues is considered, and surgery may not achieve radical (R0) resection. Nowadays, the resolution of imaging examination is so high that the vast majority of cases can be judged preoperatively and whether complete resection can be obtained. However, there are still individual patients with preoperative imaging findings that differ from the specifics of the intraoperative situation.
In Mr. Ma’s case, before surgery, the surgeon already suspected the possibility of tumor invasion based on imaging. At this point, the surgeon will fully communicate with the patient and his family, explaining what they may encounter during surgery and asking them to be psychologically prepared.
If the tumor is indeed found to be incompletely removed intraoperatively, the surgeon will also remove as many lesions and metastases as possible, depending on the circumstances. After surgery, the surgeon will also promptly explain the intraoperative specifics to the patient and family and discuss the next step in the treatment plan. It is worth clarifying that this does not involve the level of physician proficiency, but is related to the individualization of the condition.
Problem 4
What should I do if I fail to have a radical resection?
Doctors say:
For patients who had surgery for R1 or R2 resection, remedial chemotherapy or radiation therapy should be given to the residual lesions after recovery of their physical condition to control and delay recurrence, improve quality of life, and extend survival to some extent.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from a competent physician regarding your specific treatment plan.