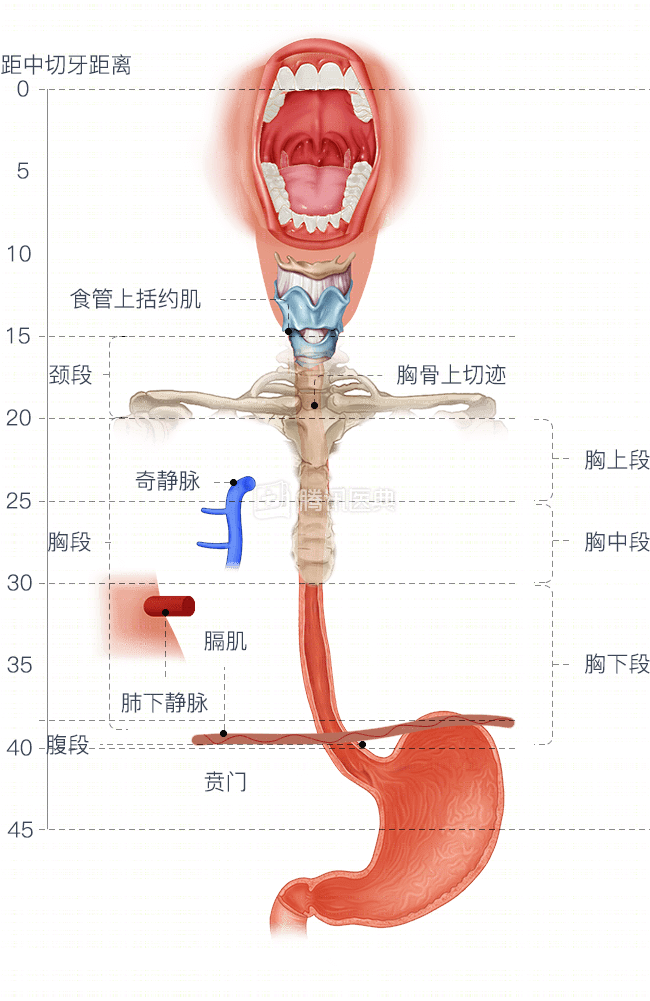
The segmentation of esophageal cancer is mainly based on the segmentation of the esophagus. According to the anatomical segmentation, the esophagus can be divided into cervical, thoracic, and abdominal segments. Clinically, the thoracic segment of the esophagus is further divided into upper thoracic, middle thoracic, and lower thoracic segments for the convenience of developing treatment plans (Figure below).
The choice of surgical approach for esophageal cancer depends precisely on the anatomy of the esophagus, the blood supply, the lymphatic network, and many other complex factors, including:
- Tumor location, length, depth of submucosal spread, and adhesions of the tumor to surrounding structures;
- The extent of planned lymph node dissection clearance;
- Selection of surrogate esophageal organs;
- Surgeon’s preference.
Radical resection for reconstruction varies slightly between sites of esophageal cancer.
- Cervical segment esophageal cancer
Cervical esophageal cancer is unique in that most patients receive primarily chemotherapy and radiation therapy. If this is not effective, or if it is judged to be surgically resectable, then a portion of the pharynx, larynx, and sub-total esophagus usually needs to be removed.
- Esophageal cancer of the thoracic segment
1. When the tumor invades the middle or lower third of the esophagus, there is a risk of “jumping metastases” in the submucosa, and subtotal esophagectomy is also usually required.
What is a “jump metastasis”? The lymph node metastasis of esophageal cancer is very jumpy, especially in the thoracic segment, which often involves lymph node metastasis outside the thoracic cavity. For example, if an esophageal cancer lesion occurs in the middle esophagus, the lymph node metastasis may occur in the abdomen or neck, or of course around the tumor in the thoracic cavity.
2. If the tumor is at the gastroesophageal junction, subtotal resection is not required.
- Esophagogastric junction or abdominal segment esophageal cancer
Traditionally, surgical treatment, i.e., partial esophagectomy, gastrectomy, or extended gastrectomy, is used.
Co-written by Dr. Li Shuang, Peking University Cancer Hospital