
Review plan
The review plan is different for patients with different stages of breast cancer. Patients with stage I-III breast cancer usually undergo surgery, followed by adjuvant chemoradiotherapy, endocrine therapy, targeted therapy, and other radical-oriented treatments. Patients with stage I-III breast cancer should have regular and regular review within 5 years after treatment. After 5 years of treatment, the patient’s risk of recurrence is reduced and the interval between reviews can be gradually extended.
| Routine Checkups | Time and remarks for examination Ask for history and physical examination |
| Ultrasound of the liver, breast area and lymphatic drainage area | According to frequency of postoperative follow-up |
| According to frequency of post-operative follow-up | |
| Mammograms and chest CT | According to frequency of post-operative follow-up |
| Check every 12 months; review shortly if abnormal findings are present | |
| Bone scan | Selected if relevant suggestive symptoms are present to exclude bone metastases |
| Breast MRI | Optional for patients undergoing breast-conserving surgery, or when supplemented by other imaging studies |
|
Gynecologic examination and gynecologic ultrasound if:
|
Checkups every 3-6 months |
| 1 time per year after baseline examination |
Stage IV breast cancer is treated to prolong survival and relieve symptoms, mostly with medical therapy such as chemotherapy, immunotherapy, targeted therapy, or endocrine therapy. Because of the high risk of progression in advanced breast cancer, systemic examinations and imaging evaluations are performed every two courses during treatment to assess treatment efficacy and detect tumor progression early. Close systemic review can be done every 2 months during targeted/endocrine maintenance therapy or discontinuation for observation.
Cautions
- Reviews should be performed as prescribed by the physician, at the time and for the items prescribed by the physician.
- At each review, bring the initial imaging and pathology reports, along with imaging films of all initial and most recent lesions, and medical records such as treatment course notes.
- Describe clearly any recent symptoms, especially new discomfort such as breast lumps, axillary lumps, fatigue, abnormal vaginal bleeding, etc.
- Any psychological problems should also be described promptly to the physician.
- Keep a record, e.g. write down the time of the next review, notes, symptoms that need extra attention according to the doctor, etc. If you need to take medication, record in detail how to take it, the duration of treatment, adverse effects and monitoring indicators.
.
Indicators to watch
Breast self-examination
Self-examination of the breast should be done on the 9th to 11th day after menstruation. First, you should face the mirror with your hands down and observe whether there is any abnormal protrusion of the breast, whether there is any depression or eczema on the skin and nipple, lift your left hand to the back of your head and check the left breast with your right hand, starting from the nipple in a circular clockwise direction and gradually moving outward until all the breasts are checked, feeling whether there is a lump in the whole breast and checking the right breast in the same way. Check the right breast in the same way. Lie flat on your back, put a pillow under your left shoulder, bend your right hand under your head and repeat the examination of both breasts. Finally, check for lymphatic enlargement in the armpit, then use your thumb and index finger to press and twist the nipple, noting any abnormal discharge.

General
Recurrence of metastasis in breast cancer can be asymptomatic in the early stages of the disease turning, and in the later stages there may be significant short-term weight loss. Breast surgery area and healthy breast lumps, regional lymph node enlargement. Lung metastasis may show dyspnea, coughing up blood, fatigue, weakness and chest pain in the later stage. Bone metastases may present with bone pain, fractures, paralysis, and other symptoms of bone metastases. Liver metastasis may present with pain in the liver area, loss of appetite, and jaundice and ascites in the late stage. Brain metastases may present with headache, altered mental status, visual impairment, etc. All types of progressively worsening symptoms need to be promptly reported to the doctor.
Imaging
Patients with breast cancer need regular postoperative follow-up ultrasound of the breast and regional lymph nodes and ultrasound of the liver. If the report suggests a new lump in the breast, a significantly enlarged axillary lymph node, or a nodule in the liver, you should promptly inform your doctor. Patients on long-term oral tamoxifen endocrine therapy are at risk of endometrial cancer. If ultrasound indicates abnormal thickening of the endometrium, you should inform your gynecologist and if necessary, perform diagnostic scraping to further clarify the diagnosis. Patients with advanced breast cancer need regular review of ultrasound, chest CT, abdominal CT, bone ECT and cranial MRI for timely detection of tumor recurrence and metastases in liver, adrenal gland, bone and brain and assessment of the efficacy of previous recurrent metastatic lesions. If the report suggests abnormalities such as enlarged lesions or new lesions, you should promptly ask your doctor to review the films to clarify the nature of the lesions and whether the tumor has recurred and metastasized or the disease has progressed.
Laboratory tests
Some patients with advanced breast cancer may have anemia, leukopenia, reduced platelets, and liver and kidney impairment due to the disease and treatment, and should also have regular follow-up blood tests and liver and kidney function after treatment to see how their organs are recovering.
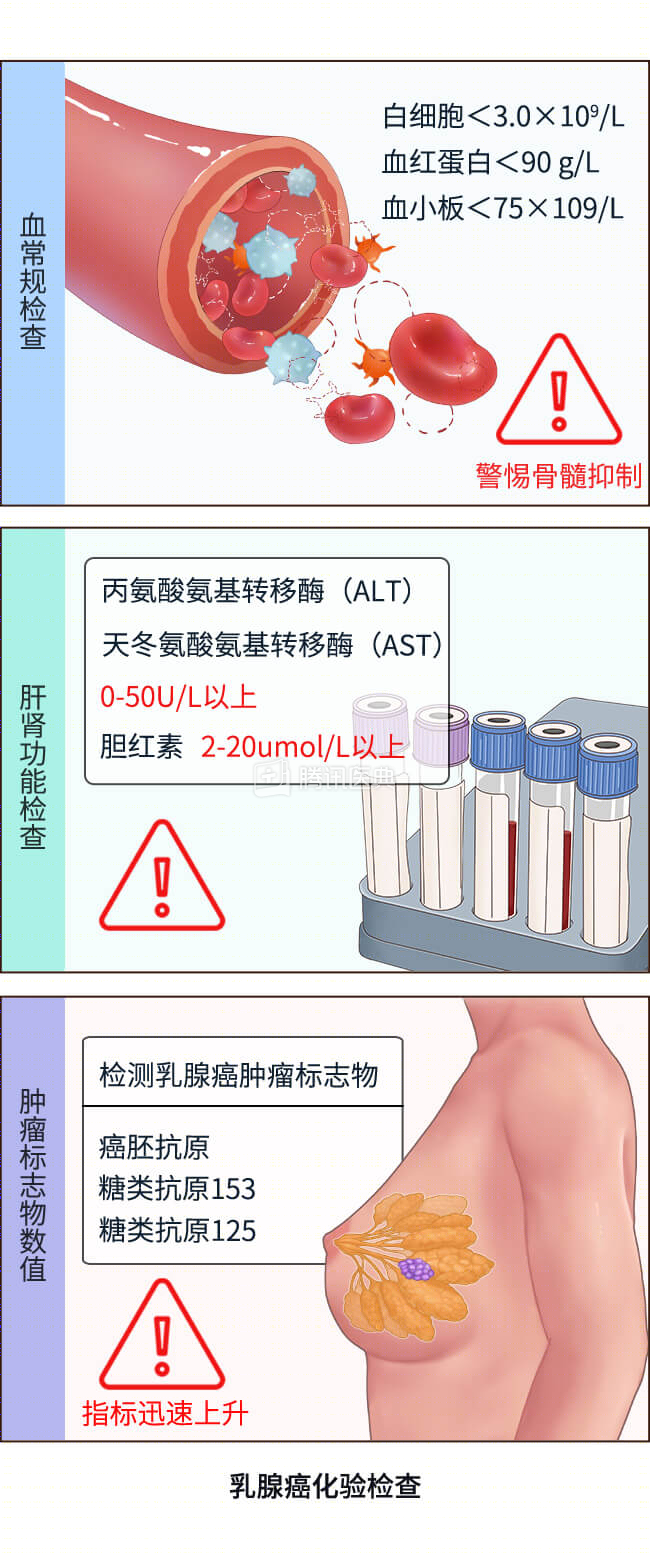
- Blood workup, alert for bone marrow suppression:
If the report shows white blood cells <3.0109/L, hemoglobin <90 g/L, and platelets <75109/L, there is a possibility of myelosuppression or other abnormalities.
Bone marrow suppression is a common adverse effect of chemotherapy in breast cancer patients. Patients often have varying degrees of hemoglobin, white blood cell, or platelet reduction, and bone marrow suppression not only delays chemotherapy, which can affect the effectiveness of treatment, but can also lead to life-threatening complications. Therefore, once the possibility of bone marrow suppression is detected, the doctor needs to be contacted for treatment at the first opportunity.
- Liver and kidney function tests to prevent liver and kidney impairment:
Abnormal elevations in alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin, as well as higher than normal creatinine on liver and kidney function tests, should alert you to the possibility of treatment-related liver and kidney impairment and require prompt consultation with your physician for further testing.
- Tumor marker values to watch:
Patients with breast cancer need to be tested for breast cancer tumor markers, such as carcinoembryonic antigen, glycoantigen 153, glycoantigen 125, etc., which correlate with tumor disease.