The annual medical checkup is an ordeal for every normal person, and it always feels like a mountain of rain and wind when faced with a bunch of numbers and arrows.
The most common question asked in the urology office is about prostate specific antigen (PSA), a blood test that is listed among the tumor-related markers, so patients enter the urology office with anxiety and anxiety to be “judged” by the doctor. “The patient enters the urology office with anxiety and anxiety. Doctors usually encounter two types of patients in the clinic:
- Patients who feel that they may be far away from prostate cancer, or they may be one step away and are afraid to know the truth, so they choose to avoid it;
- The other is to feel that you may already have prostate cancer and just wait for the doctor’s “verdict” and choose to dance with the cancer.
I have had many patients with elevated PSA, and the following two patients have a different approach to life that is very memorable.
Case 1: Refusal of puncture biopsy after elevated PSA developed into bone metastasis of prostate cancer 4 years later
Tan XX, in a physical examination organized by his unit one year before retirement, was found PSA 5.6ng/ml, after repeated urging from his wife to come to the hospital, I carefully asked him about his usual urination and performed a routine rectal examination, and found a hard nodule in the left lobe of his prostate. The patient’s condition was not found to be a hard nodule in the left lobe of the prostate.
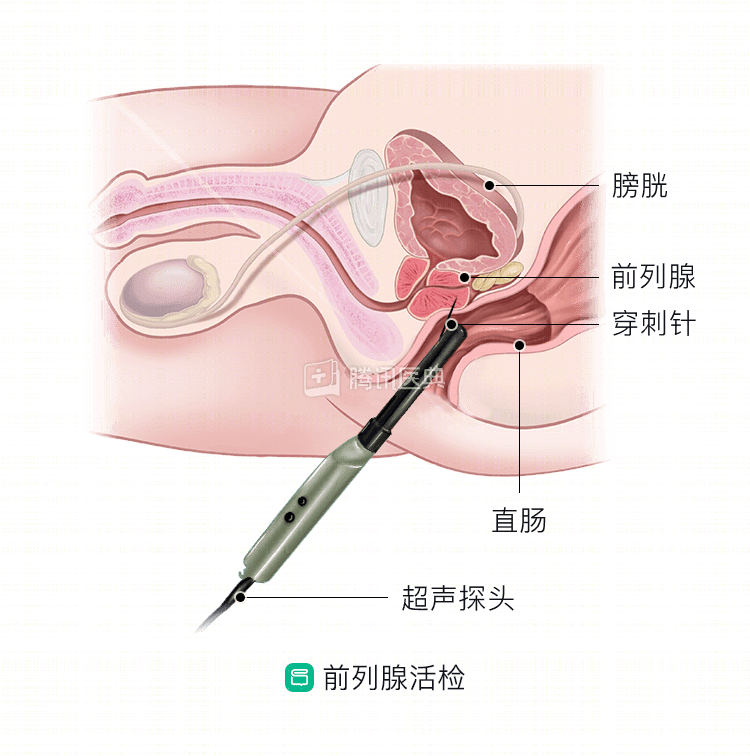
As I expected, the rectal ultrasound suggested that there was indeed a hypoechoic nodule in the left peripheral zone of the prostate, for which a puncture biopsy was necessary, but Mr. Tan stubbornly chose to avoid and leave it to chance.
Four years later, when Mr. Tan came to our clinic for help again with pain in his lower back, the examination revealed that his PSA index had risen above 800, and a bone scan showed multiple bone metastases throughout his body.
Case 2: Prostate cancer was found after regular PSA examination, and after timely radical treatment, everything is good for 8 years and has reached cure
.
Liu XX, who has been undergoing medical checkups since he was 50 years old, paying particular attention to his tumor markers, found an abnormal PSA of 4.5ng/ml in his fifth year of medical checkups. although he had abdominal ultrasound every time to check the size and echogenicity of his prostate, this abnormal blood indicator made him accept my suggestion to add rectal ultrasound and MRI.
The results clearly suggested an abnormal signal in the right peripheral zone of the prostate, and two days later Mr. Liu underwent a rectal ultrasound-guided multi-point puncture biopsy of the prostate, and the pathology report showed adenocarcinoma of the prostate with a Gleson grade of 3+3.
Fortunately, Mr. Liu underwent immediate laparoscopic radical prostatectomy, and because of the timely detection and complete surgical cure, the patient has been followed up for eight years now, with all indicators showing good results and meeting the criteria for complete cure.
After reading the above two case presentations of prostate cancer, many patients must have many questions and misconceptions, such as:
- Does a blood PSA greater than 4ng/ml above normal mean that you have prostate cancer?
- Why do I have a prostate puncture biopsy when my blood PSA is abnormal and my rectal ultrasound and MRI suggest a tumor in the prostate?
- Does a prostate puncture biopsy find no prostate cancer and everything is fine?
These questions and misconceptions need to be answered from a professional perspective by our expert urologists.
- First, when PSA s are elevated and greater than normal, it does not necessarily mean that you have prostate malignancy. The most common patients with prostate enlargement and prostatitis also have elevated blood PSA, and although we call PSA a prostate-specific antigen, it is not specific to prostate cancer, and only if other ancillary tests reveal abnormalities is there a high degree of suspicion that prostate cancer is present.
- Second, although all of the laboratory results and ancillary tests point to suspicion of prostate cancer, these are only clinical diagnoses based on the combination of the physician’s experience and the results of the tests, and are not the final diagnosis. The final pathologic diagnosis is needed to confirm the diagnosis, and how to obtain it? That requires a puncture of the prostate tissue, and the tissue obtained from the puncture is sent to the pathology department for pathological diagnosis. Therefore puncture biopsy is the “gold standard” for prostate cancer diagnosis, a higher standard of diagnosis and basis than clinical diagnosis.
- Also, although prostate puncture biopsy is the “gold standard” for diagnosing prostate cancer, it is not 100% accurate. If the tumor tissue is small at the time of the puncture and the puncture needle does not capture the tumor tissue, the final pathological diagnosis will be inaccurate. Experienced physicians will analyze the results of the puncture and will not easily trust the results of the puncture. If the patient’s blood PSA is still further elevated, the physician will remind the patient to have another puncture for a larger, more precise strike on the suspicious site and to obtain a valuable diagnosis, which is why there are individual patients who have repeated multiple puncture biopsies.
- Finally, many patients have concerns about the puncture biopsy method and are reluctant to undergo this diagnostic method because they fear that it may cause the spread and metastasis of tumor cells. The actual fact is that the needle is very fine and the tissue is cut in the prostate gland, and the cutting time is short and the damage is minimal, so there is no need to worry about the implantation and spread of tumor cells.
Prostate cancer has become the most prevalent tumor in men in Europe and the United States, and has surpassed lung cancer as the number one malignancy in men in China. Despite its increasing incidence year by year, it is now increasingly seen as a “chronic disease” in the field of oncology that can be cured or managed.
Blood PSA testing is becoming a screening indicator for prostate cancer, and routine blood tests are recommended once a year for men over the age of 40. If there are abnormalities, the interval between blood PSA tests can be shortened to once every six months or three months, and early intervention with ancillary tests and punctures can be used to detect prostate cancer early.
Related articles: