Early-stage esophageal cancer can usually be treated endoscopically to obtain radical cure. In general, endoscopic resection can be performed if you have no lymph node metastases, or very low metastases. If there are conditions such as advanced age or poor health that prevent you from tolerating endoscopic resection, or if you do not want to have endoscopic resection, then endoscopic non-excisional treatment is an option.
In this article, we will show, through a case study, what conditions can be selected for endoscopic non-excisional treatment and how the treatment plan was developed.
Mr. Li, 75 years old, has a 50-plus-year history of alcohol consumption and smoking, a 20-plus-year history of hypertension, a 30-plus-year history of diabetes, a coronary stent placement two years ago, and a daily need for oral aspirin and other medications. In recent days, he came to the Endoscopy Center of Peking University Cancer Hospital with acid reflux and heartburn for up to 1 month.
Diagnostic process
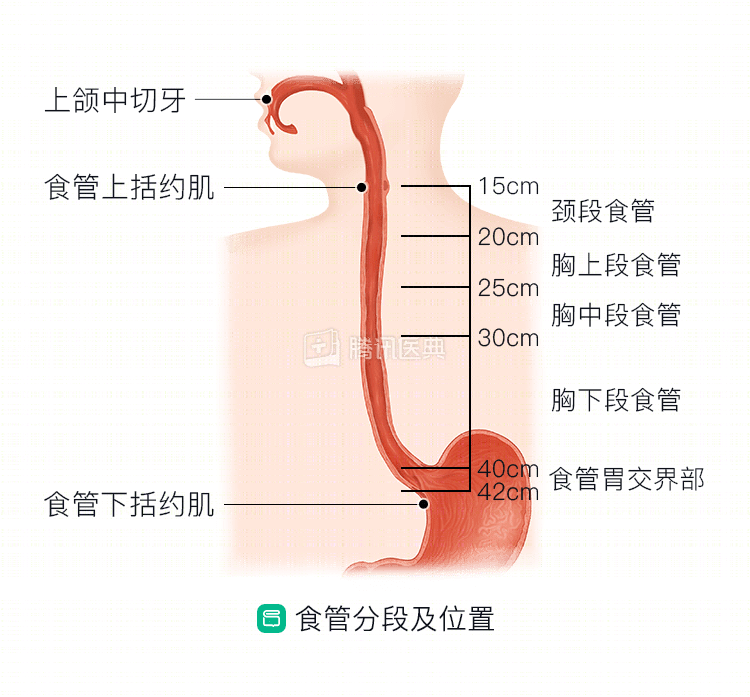
Mr. Li underwent a general gastroscopy in the outpatient clinic. The doctor found a flat lesion in the left wall of the esophagus 30-33 cm from the incisors (incisors) under the scope, and suspected the presence of a neoplastic esophageal lesion.
Subsequently, the physician considered the lesion to be consistent with early esophageal cancer by magnifying endoscopy with narrow-band imaging (NBI-ME) and ultrasound endoscopy.
After endoscopy, the physician sent the tissue sample to the pathology department, where the diagnosis of “highly differentiated esophageal squamous cell carcinoma” was confirmed.
To further determine whether the cancer was early and whether there were lymph node metastases, the doctor prescribed additional tests for Mr. Li. In the end, the chest enhancement CT revealed no significant thickening of the esophageal wall and no obvious enlarged lymph nodes around the esophagus; the abdominopelvic enhancement CT also found no significant abnormalities. The clinical stage was cT1N0M0 stage IA.
Looking at this code-like string of diagnostic results, Mr. Li was completely confused.
The endoscopist explained to him that “c” refers to clinical stage, and stage IA means early stage; “T” stands for tumor, which describes the size and extent of the tumor lesion, and T1 refers to the tumor invading the esophageal mucosa or submucosa. The “N” stands for Lymph Node, N0 means no metastasis in the peri-esophageal lymph nodes; “M” stands for Metastasis, M0 means no distant metastasis.
And highly differentiated cancer means that the cancer cells are less malignant and the expected outcome of treatment is better.
That is, Mr. Li’s esophageal cancer was located in the mucosal layer of the esophagus, with minimal risk of lymph node metastasis, and met the indications for endoscopic resection.
Treatment plan selection
In Mr. Li’s case, the first choice would be endoscopic resection. However, he is 75 years old, a senior patient, and has his own combination of chronic diseases such as hypertension, diabetes, and coronary artery disease, and his physical condition is not very good overall.
When they heard the doctor say that endoscopic resection would require general anesthesia and that anesthesia might be risky, his family was very concerned, fearing that Mr. Li would not be able to tolerate the risk of being “cut” in his body and having general anesthesia, so they were reluctant to opt for such an invasive treatment.
After listening to the family, the doctor decided to use photodynamic therapy, an endoscopic, non-excisional treatment.
Photodynamic therapy has a number of advantages over endoscopic resection:
- Minimal trauma and quick recovery. It basically does not interfere with normal diet during the treatment.
- Targeted killing.
- Targeted killing of tumors with minimal damage to normal tissues surrounding the lesion. This selective killing effect is difficult to be achieved by many other treatments.
- Good applicability. Photodynamic therapy is effective on cancerous tissues of different cell types and has a wide range of applicability.
- If residual lesions are found or new lesions appear after treatment, the treatment can be repeated.
- For patients who cannot undergo surgical resection, such as those of advanced age, cardiopulmonary, hepatic and renal insufficiency, and hemophilia, photodynamic therapy can effectively reduce pain and improve the quality of life.
- No anesthesia is required, and the treatment can be done in an outpatient clinic, and the treatment effect is no worse than endoscopic resection.
To learn more about photodynamic therapy, please read:
However, no treatment can have only advantages and no disadvantages. Doctors were also honest with Mr. Li and his family: photodynamic therapy does not allow for specimens from the lesion site, which would not allow for accurate pathological evaluation or clarity on whether the tumor has been completely removed.
There was a point of concern raised by Mr. Li himself: if the pathology cannot be accurately assessed and it is not clear whether the cut is clean, is photodynamic therapy prone to recurrence?
The doctor said:
Although Mr. Li is suitable for photodynamic therapy in terms of clinical staging, it can only kill cancer cells close to the inner surface of the esophagus, but not those that have penetrated deeper into the esophagus or other organs, because the light-activated drug must be activated by light to take effect. This requires Mr. Li to come to the hospital for regular review of gastroscopy. Once a recurrence is detected, it should be treated as soon as possible.
After hearing this explanation, Mr. Li and his family had another detailed and thorough communication with the doctor and finally agreed to use photodynamic therapy.
The treatment process
There are several visits to the Endoscopy Center to complete the photodynamic therapy, and the main steps are as follows: 24-hour advance injection of the photoactivating drug – the first formal treatment – and the second formal treatment approximately 48 hours later.
- Before treatment, the doctor controlled Mr. Li’s blood pressure and blood glucose within reasonable limits with treatment and stopped antiplatelet drugs such as aspirin for about 1 week.
- Related tests for cardiopulmonary function were refined to ensure that the risk was minimized.
- Twenty-four hours before treatment, Mr. Li came to the Endoscopy Center clinic for a photoactivated drug injection. The nurse first gave him a skin test for the photoactivator, and after 15-20 minutes of observation, he was judged to be negative before the photoactivator was given intravenously. The procedure was very simple, just like a hangnail, injecting photosensitizer into the body. The nurse also gave Mr. Li a brief explanation: photosensitizers themselves do not have tumor-killing effects, but rather use laser light for excitation to cause irreversible damage to tumor cell membranes, mitochondria, lysosomes and other structures, ultimately leading to the death of cancer cells.
- After the drug injection, the doctor instructed Mr. Li to put on sunglasses in time to avoid all strong stimulating light sources, and it is best not to go out. After going home, he could eat foods high in protein, calories and vitamins to strengthen his resistance. Then, Mr. Li went home to rest. Next, the light-activated drugs will slowly gather in the cancerous tissue.
- The night before the official treatment, he did not eat as prescribed, making sure he fasted for at least 6 hours. This is because it is important to keep the esophagus and stomach clean and free of food debris during endoscopic treatment to ensure that the lesions on the esophageal mucosa are clearly visible.
- On the day of treatment, Mr. Li came to the endoscopy clinic. He entered a special dark room for photodynamic therapy. Through the endoscope, the doctor aims a special laser at the lesion, causing changes in the photosensitizers gathered in the cancer cells, producing a variety of reactive oxygen species that directly kill the tumor cells; at the same time, it causes damage to the tumor blood vessels and affects the blood supply to the tumor. Most importantly, this treatment causes minimal damage to the surrounding normal tissues.
- About 15 to 20 minutes later, the illumination ended, and the doctor slowly withdrew the gastroscope and the light-guided fiber from Mr. Li’s body after looking around the lesion through the gastroscope and seeing no obvious bleeding, ending the treatment. Throughout the process, the doctor monitored his vital signs and there were no abnormalities, and Mr. Li felt no other discomfort. The doctor instructed him to make sure his body was completely covered when he went home to avoid all possibility of direct exposure to sunlight. 48 hours later, he would return to repeat the treatment. Avoid sun exposure for 30 days after treatment to prevent the development of photoallergic dermatitis.
- 48 hours later, Mr. Li came to the hospital as scheduled to continue photodynamic therapy. Through gastroscopy, the physician found evidence of tissue necrosis in the location of the lesion, which indicated that the first treatment was effective. After the necrotic tissue was removed, the physician performed a second photodynamic therapy and instructed Mr. Li that the post-treatment precautions were the same as the previous treatment.
- For 1 week after treatment, Mr. Li had a brief period of dysphagia. The doctor had already told him before treatment that this was probably due to swelling of the esophagus after treatment and that no special treatment was usually needed. Sure enough, as the edema slowly subsided, the swallowing discomfort gradually subsided.
.
Postoperative review
One month after the end of treatment, Mr. Li came in for his first gastroscopy review and found that the lesion had disappeared.
Subsequently, he followed the doctor’s advice to follow up his treatment with a strict frequency of gastroscopy review every 3 months, and none of the lesions were found to have recurred.
Currently, Mr. Li has been undergoing photodynamic therapy for 1 year, has no significant discomfort, is able to eat and drink normally, and is still adhering to regular follow-up visits.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from a competent physician regarding your specific treatment plan.