
There are a variety of surgical options for breast cancer, and surgeons will make specific choices based on individual circumstances. For example, some lesions can be removed precisely while preserving breast appearance and function with breast-conserving surgery, axillary lymph node dissection may be avoided with sentinel lymph node biopsy, and there are minimally invasive lumpectomy techniques that allow removal of internal breast lymph nodes without removing the rib cartilage.
This article takes a look at what surgical options are available for breast cancer, which may help to allay preoperative concerns and prepare you for the procedure.
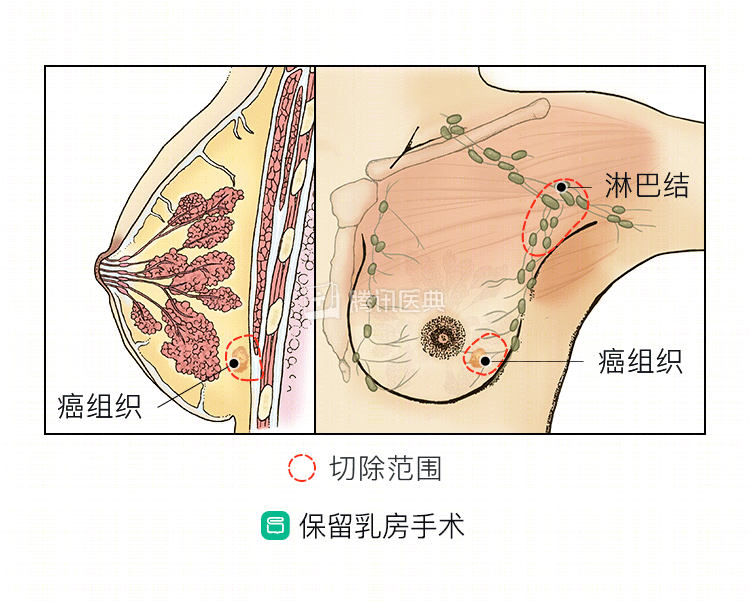
Breast-conserving surgery
Breast-conserving surgery is the best option for local treatment of breast cancer if you are eligible for breast conservation. Breast-conserving surgery is usually preceded by a mammogram and magnetic resonance imaging (MRI) to rule out multiple and separately extensive tumors.
During surgery, the surgeon makes an incision of the appropriate length in the skin on the surface of the tumor, or, for more aesthetic reasons, may use an incision along the areola if available.
Through the skin incision, the surgeon removes the tumor and some of the surrounding normal glands intact, and then marks the five margins of the excised tissue: inner, outer, upper, lower, and bottom, and sends it for rapid frozen pathology to determine that the tumor was removed completely without residue. If the margins are positive, the surgeon will extend the resection in that direction and send it for frozen pathology again. If it is still positive, the tumor is extensive and no longer suitable for breast conservation and a mastectomy is required. Finally, the surgeon will reshape the breast in an appropriate manner, suture the incision, and leave drainage in place if necessary.
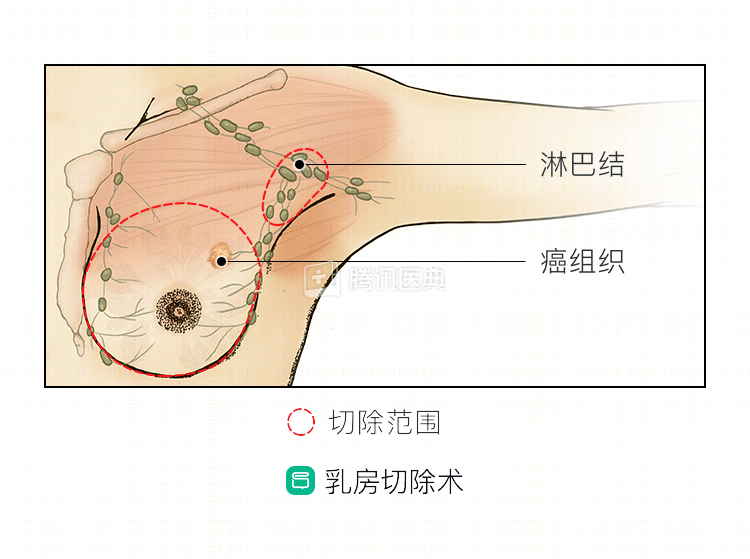
Mastectomy
If the tumor can be surgically removed but does not meet the conditions for breast conservation, mastectomy would be the only option. In general, these tumors are often large and locally staged slightly late.
At the time of surgery, the surgeon usually makes a shuttle-shaped incision to include the skin on the surface of the tumor and the nipple areola. If the patient has a need for breast reconstruction and the nipple areola is not invaded by the tumor, the surgeon may also consider preserving the nipple areola. In some patients, mastectomy may also be accomplished lumpectomatically, which requires only 3 small 1-cm incisions on the side of the chest.
The procedure preserves only a thin layer of fat under the skin, from which the entire breast is removed down to the surface of the muscles (pectoralis major and serratus anterior). After the lymph nodes are treated, the surgeon usually leaves a drain in place and closes the incision. If the tumor is large, more skin is removed, and the incision cannot be sutured directly, a skin graft may be placed.
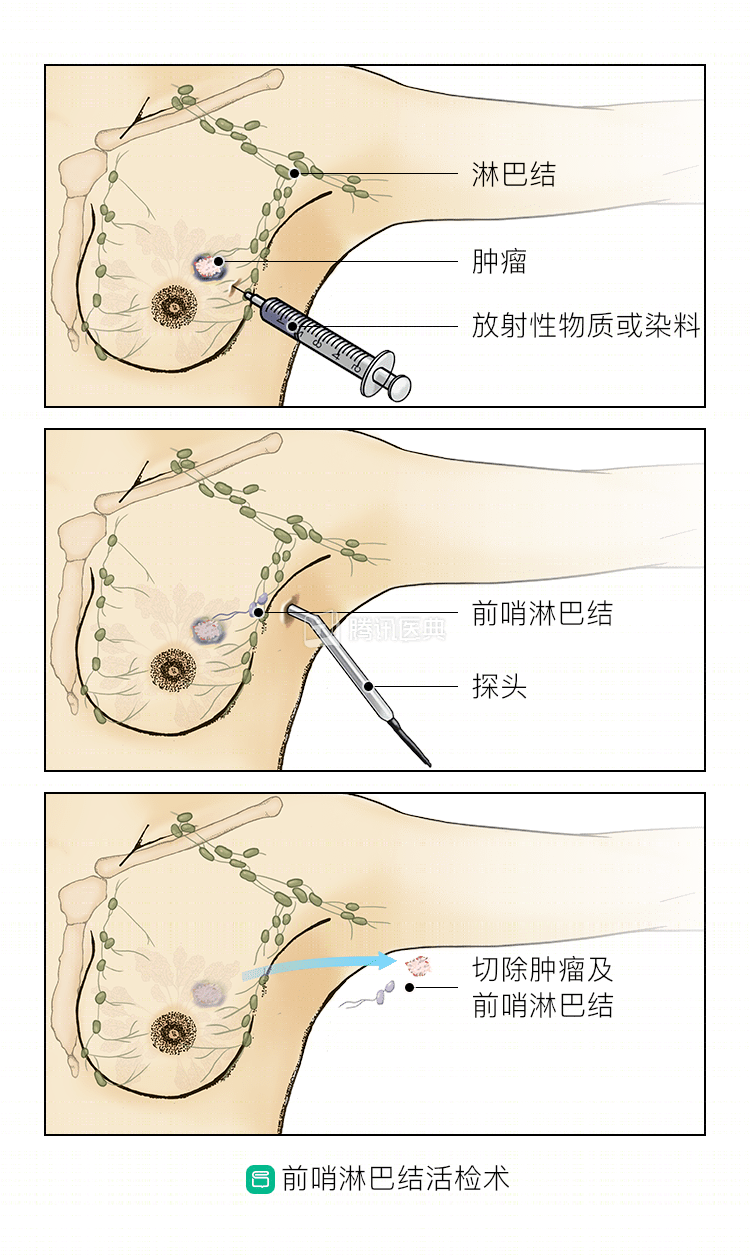
Aposterior lymph node biopsy
In the vast majority of cases, an anterior sentinel lymph node biopsy can accurately determine the status of axillary lymph nodes and thus may be able to avoid the complications associated with axillary lymph node dissection, and therefore it is often used by physicians as the preferred lymph node procedure for those with no axillary lymph node metastases on clinical examination.
Before surgery, the surgeon will inject an appropriate amount of tracer around the tumor or the nipple areola area to stain the sentinel lymph nodes, sometimes using a combination of two dyes to allow for more accurate visualization of the sentinel lymph nodes.
Intraoperatively, the surgeon identifies the stained lymph node, the sentinel lymph node, either by instrument or by visual inspection, and sends it for rapid frozen pathology. If there are no metastases in the sentinel lymph nodes, axillary lymph node dissection is not necessary, and even recent studies suggest that axillary radiation therapy given to those with only 1 or 2 metastases in the sentinel lymph nodes is equivalent to local control with dissection surgery.
Axillary lymph node dissection
Axillary lymph node dissection is necessary for those with metastases in the axillary lymph nodes. Through a breast or axillary incision, the surgeon will remove the lymphatic fatty tissue of the axilla along with the nerves and blood vessels of the axilla, while protecting them. If metastasis is suspected in the subclavian lymph nodes, the surgeon will continue with the debridement. Finally, the surgeon will place a drainage tube to close the incision.
Internal breast lymph node biopsy or dissection
Conventional internal mammary lymph node biopsies are performed by cutting the muscle between the ribs above to find and remove the lymph nodes, which usually requires cutting through the rib cartilage to do so, but this approach can destabilize the thorax. Currently, this can be accomplished through a minimally invasive lumpectomy technique with 3 small holes in the lateral chest wall, using a thoracoscopic or surgical robotic system to remove the lymph nodes intact from the chest cavity.
The postoperative period requires only a few days of drainage of the chest cavity, which is less invasive and results in a faster recovery without compromising the integrity and stability of the thorax.
Mastopexy
For breast loss brought on by mastectomy, and for breast loss brought on by extensive breast-conserving surgery to remove a tumor, breast reconstruction surgery can be used to recreate the appearance of the breast.
- Implants are a common source of reconstructive material. An implant of the appropriate volume and shape (round or teardrop) is typically placed in the appropriate position in the breast after mastectomy.
- Autologous tissue graft reconstruction is another method. The surgeon will cut tissue with an intact blood supply (e.g., rectus abdominis flap, latissimus dorsi flap, greater omentum, etc.) at the appropriate site (donor area) and transfer it to the area of breast deficiency to reshape it into a new breast shape.
- Breast reconstruction is also possible through autologous fat injection, in which fat is taken from fat-rich areas such as the abdomen, thighs, and buttocks, processed to obtain appropriate fat particles, and then injected into the missing area of the breast. Typically, due to the large volume of the breast, autologous fat grafting requires multiple procedures to obtain the proper volume and may end up requiring a revision surgery to create the perfect shape.
In today’s highly advanced surgical technology, breast cancer surgical approaches have more options and are becoming more refined and precise. As a patient, you can fully communicate with your doctor and choose the surgical option that suits your condition and needs (with the participation of Dr. Yang Shih, attending surgeon of Breast and Thyroid Surgery at Southwest Hospital of Army Medical University)