For patients with early-stage prostate cancer, radical prostatectomy can serve the purpose of completely removing the cancer cells; for patients with intermediate and advanced stages, radical prostatectomy can serve the purpose of reducing the tumor load.
Because of the lack of a “clear-cut” prostate and the variation in surgeon experience, some patients may have residual marginal disease, positive lymph nodes, and microscopic metastases that are not visible to the naked eye, so postoperative adjuvant therapy can improve long-term survival for these patients.
Who are the appropriate patients for postoperative adjuvant therapy?
Patients who need postoperative adjuvant therapy
Patients who require postoperative adjuvant therapy have the following characteristics:
- Postoperative pathology with positive cut margins;
- Postoperative pathology suggestive of positive cleared down lymph nodes;
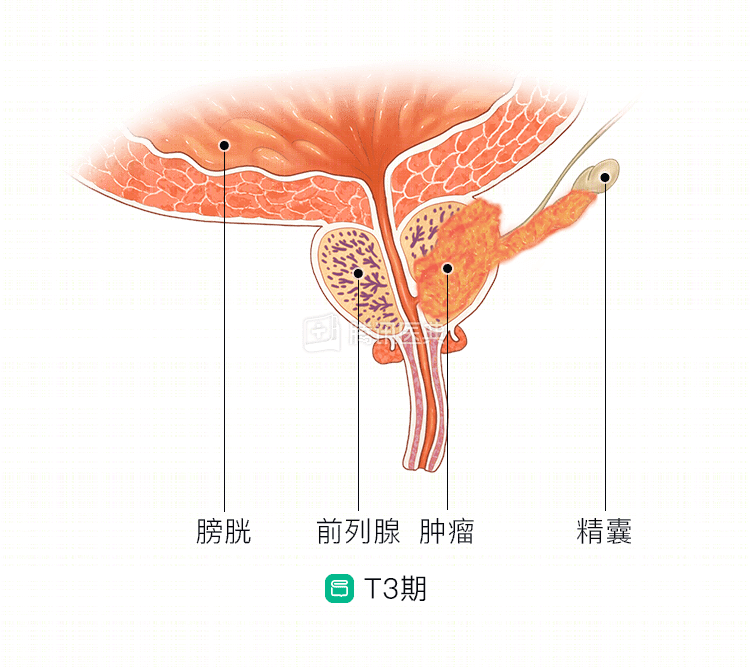
- Postoperative pathology suggesting breakthrough of the envelope or invasion of the seminal vesicles (pT3 stage);
- Pre-operative presence of high-risk factors: Gleason score greater than 7, PSA greater than 20ng/ml.
What are the common options for postoperative adjuvant therapy?
Adjunctive treatment modalities include the following:
1. anti-androgen therapy
The use of androgen receptor antagonists to inhibit androgen stimulation of prostate cancer cells.
Commonly used oral drugs: flutamide, bicalutamide. The recently developed and clinically used androgen biosynthesis inhibitor, abiraterone, provides another powerful weapon and is already covered by health insurance.
2. pharmacological depot or surgical depot
“Depotting” is also known as “depotting”, and as the name implies, it is the removal of androgens, both chemically and surgically.
The chemical method is the use of drugs for the purpose of debulking, commonly used drugs such as Inhibiton (leuprolide acetate microspheres for injection) and Noradren (goserelin acetate extended release implant).
Surgical debridement refers to the removal of the patient’s testes bilaterally to achieve debridement in a single session.
3. Maximal androgen blockade
The common approach is to use a combination of “anti-androgen” + “depot” to remove or block androgens of testicular and adrenal origin.
Related reading: