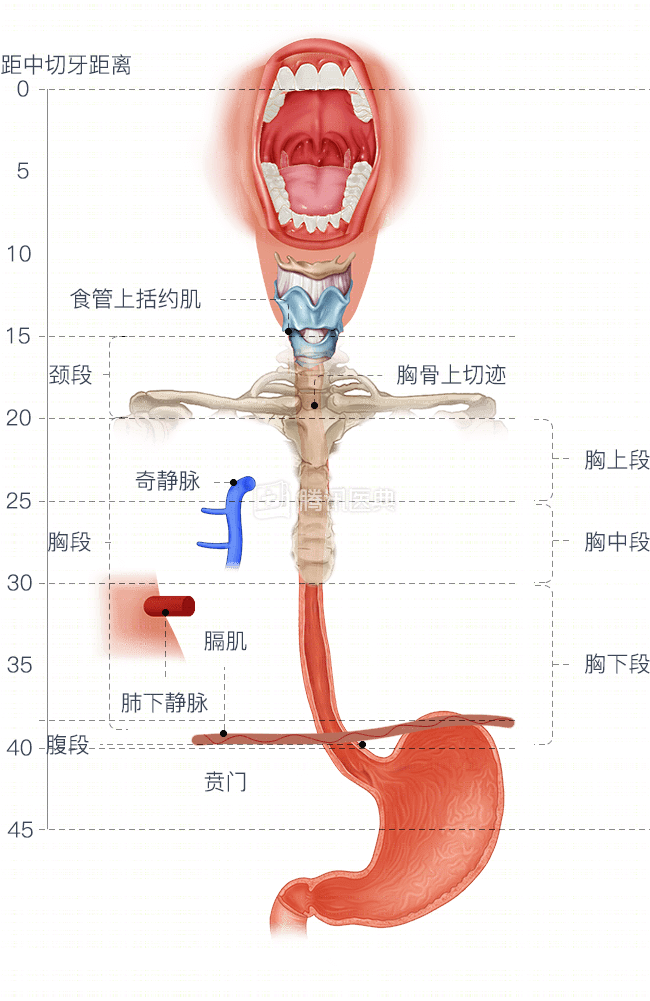
Cervical esophageal carcinoma (CEC) occurs between the lower border of the cricoid cartilage and the superior sternal notch, the part of the esophagus that does not enter the thoracic cavity.
The incidence of cervical esophageal cancer is low, accounting for 2% to 10% of all esophageal cancers. It is mainly squamous carcinoma. The onset of the disease is mostly at a locally advanced stage, with heavy dysphagia symptoms. Since the lesion is close to important organs such as larynx, trachea and thyroid gland, surgery is very difficult and traumatic. Radical radiotherapy is currently recommended as the standard treatment modality for CEC, which preserves organ function. Dosimetric and organ preservation considerations suggest that intensity-modulated radiotherapy is superior to 3D conformal radiotherapy.
To learn more about radiotherapy techniques such as intensity-modulated radiotherapy, read the following articles:
In this article, we use a typical case to illustrate how doctors choose treatment options when facing cervical esophageal cancer.
Mr. Fang, 47 years old. presented in April 2017 with pain in the pharynx and loss of appetite. After taking medication on his own for about a month, his symptoms did not resolve, and he also developed intermittent dysphagia with increased pain, which was more pronounced when eating coarse foods and required water to help swallow.
By chance, he felt a lump on the left side of his neck that was tough and hard, without pressure or pain, and with little mobility. After observing the mass for some time, he noticed an increase in size, about 4×4 cm, and an unexplained fever of up to 38.5°C. Mr. Fang visited the hospital in May 2017.
Diagnostic process
Gastroscopy suggested: 16 cm from the incisor, the esophageal mucosa showed irregular hyperplasia with a congested and eroded surface and poor elasticity, making the gastroscope impossible to pass. The physician took a biopsy under endoscopy and sent it for pathological examination.
The pathology report suggested: highly differentiated squamous carcinoma of the cervical segment of the esophagus.
On the advice of his doctor, Mr. Fang completed a series of tests.
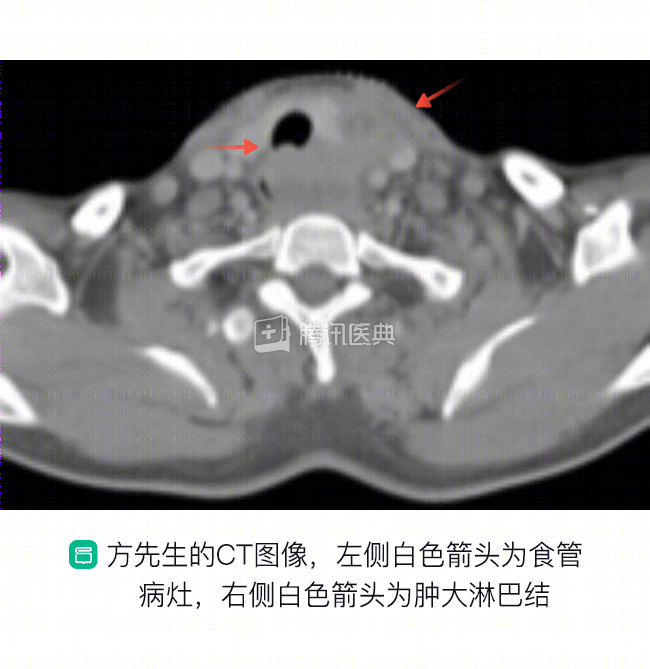
CT of the neck revealed thickening of the wall of the cervical esophagus and a localized irregular soft tissue mass measuring about 35x30mm.
Enhanced CT scan suggests: the outer esophageal membrane is blurred, the surrounding fatty interstitial space is dense, and the mass compresses the anterior trachea with marked deformation and protrudes into the tracheal lumen. The left supraclavicular region showed enlarged lymph nodes, the larger of which was approximately 16x10mm; on the right supraclavicular region and bilaterally next to the carotid sheath, multiple small lymph nodes, all smaller than 10mm, were found.
Upper gastrointestinal tract imaging suggests: An irregular filling defect with mucosal disturbance and disruption is seen in the cervical esophagus, and a niche is seen within (i.e., a concave area at the site of the broken lesion that appears abnormally raised after barium filling, like a Buddhist niche). The lesion is about 6.5 cm long. barium passage is slightly obstructed.
Both chest CT and abdominal ultrasound showed no abnormalities, indicating that the lesion did not invade the thoracic esophagus, nor did it have liver or lung metastases.
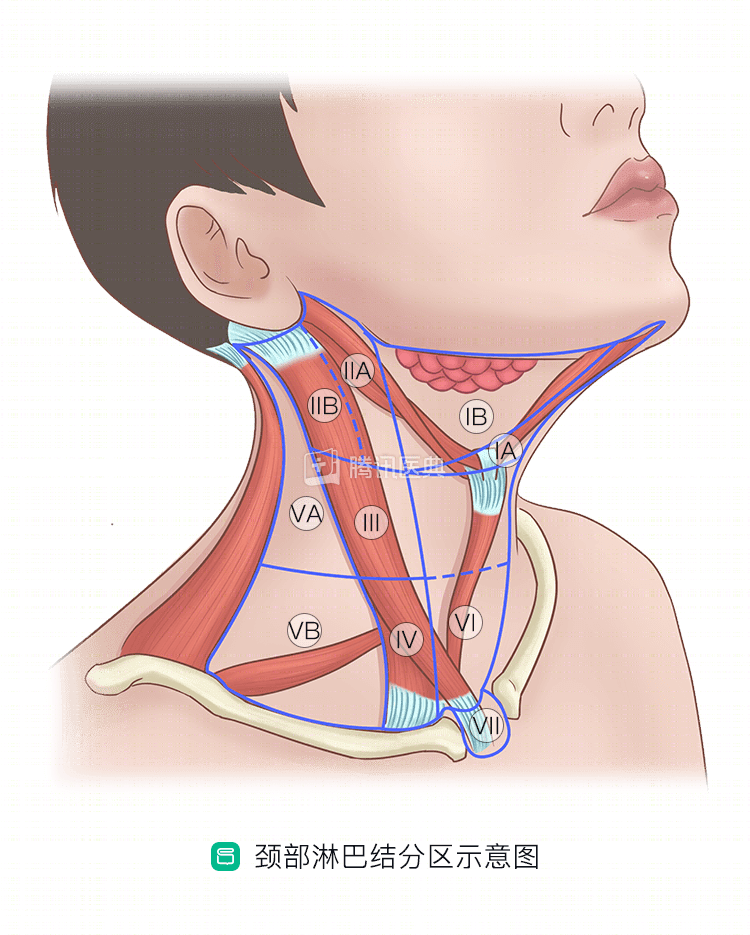
In combination with the above findings, the physician made the diagnosis: highly differentiated squamous carcinoma of the cervical esophagus, clinical stage III, which has invaded the trachea, thyroid, etc.; lymph node metastasis in the left III, IV, Vb, and bilateral VIb areas. The cervical lymph nodes (below) are divided into 10 regions, of which, III, IV, and Vb are roughly in the posterior aspect of the lower middle neck, region VIb is roughly the posterior tracheal, paraesophageal lymph nodes.
Treatment plan development
After diagnosis, Mr. Fang’s case was discussed by the multidisciplinary team, and the results were communicated to him and his family.
The doctor said:
Your esophageal cancer lesion is located in the cervical segment, invading the posterior wall of the trachea and the thyroid gland, with multiple metastatic lymph nodes in the neck, and is locally advanced.
The invasion of the posterior wall of the trachea means that complete surgical resection is difficult, and surgery is not certain to perform radical resection; radical radiotherapy is recommended.
However, radiotherapy can lead to a more severe tracheal response, with possible risks of neck tissue edema, choking, and bleeding, as well as adverse effects such as malaise, nausea and vomiting, radiation esophagitis, and radiation dermatitis, briefly causing more difficulty in eating via the mouth and aggravating malnutrition. And poor nutritional status may lead to interruption of treatment. Therefore, endoscopically assisted placement of a nasogastric tube for nutritional support via enteral nutrition is recommended first.
Mr. Fang and his family followed the doctor’s advice, agreed to receive radiotherapy as well as tube placement, and signed an informed consent form.
After supportive treatment including anti-inflammatory and nutritional therapy, his temperature recovered and his general condition improved, and he began treatment as planned.
Treatment course
In June 2017, Mr. Fang began radical radiation therapy, which will be done 33 times in total and last 6 1/2 weeks. He had 1 radiation treatment per day, Monday through Friday, with Saturday and Sunday off.
During radiation therapy, 2 cycles of cisplatin single-agent concurrent chemotherapy (an infusion of 80 mg/m on day 1 and a 21-day cycle, or a 3-week regimen) were also completed.
Mr. Fang also had weekly follow-up blood tests, blood biochemistry, and other indicators to monitor for adverse effects of radiotherapy.
After completing week 1 of concurrent chemotherapy and 15 radiation treatments, he felt his neck lump had shrunk and his difficulty in swallowing had subsided from before.
A repeat CT after 20 radiation treatments showed significant lesion shrinkage, so his treatment plan was modified to reduce the scope of radiation therapy to reduce damage to surrounding normal tissue.
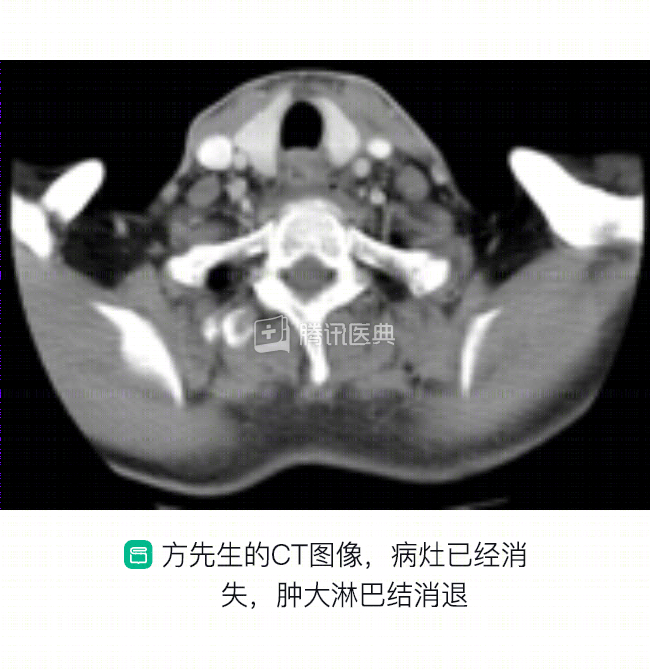
After the completion of radiotherapy, Mr. Fang’s cervical esophageal lesion and cervical lymph nodes were significantly smaller, and he was able to eat significantly more freely than before without any discomfort such as painful swallowing or fever.
He followed his doctor’s orders and insisted on regular follow-ups (every 3 months), and there have been no signs of recurrence since.
Summary
With Mr. Fang’s example, we can summarize the treatment idea of CEC:
First, the location of the lesion was clarified by gastroscopy and a pathological diagnosis was obtained. Then, the upper gastrointestinal tract imaging was improved to clarify the lesion length and degree of stenosis; the cervicothoracic CT was improved to clarify the degree of local lesion invasion and lymph node metastasis; and the abdominal examination was improved to clarify the status of distant metastasis.
After staging is clarified, the possibility of surgery is evaluated. CEC confined to the mucosa can be treated by endoscopic submucosal dissection (ESD); other stages of CEC are inoperable due to high location, complex surrounding structures, and lack of sufficient normal esophagus for anastomosis after resection of the lesion. The current clinical recommendation is that radical radiotherapy for locally advanced CEC has a 5-year survival rate of approximately 25% to 55%. During treatment, it is important to strengthen the monitoring of adverse effects and timely symptomatic management to minimize normal tissue damage.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be individualized, and this case does not represent a “like patient” treatment decision. Please seek professional advice from a competent physician regarding your specific treatment plan.
Co-Author: Dr. Yangzi Zhang, Peking University Cancer Hospital