Immunotherapy has made some progress in the treatment of esophageal cancer. But overall, there is no immunotherapy approach that has been approved for use in the treatment of esophageal cancer. And, not all patients with esophageal cancer can benefit from it.
Immunotherapy is not a miracle drug, and it’s important to screen the “beneficiary population” for effectiveness
.
According to early clinical trial data, PD-1/PD-L1 monoclonal antibody-based immunotherapy is 17% effective in esophageal cancer; even in screened PD-L1-positive patients, it is only 28% effective. But these lucky treatment-effective individuals get a very clear survival benefit, so screening the target population is the way forward for immunotherapy.
So how can your doctor tell if you are one of the lucky ones who will be “favored” by immunotherapy? It depends on a number of markers.
Markers that have been identified that may benefit from immunotherapy include: high PD-L1 expression, high Tumor Mutation Burden (TMB), tumor microsatellite instability (MSI) tumor-infiltrating lymphocytes, and neoantigen content. lymphocytes, high neoantigen content, etc. The majority of these markers are detected by blood tests, which are often referred to as “genetic tests.
1. PD-L1 expression level
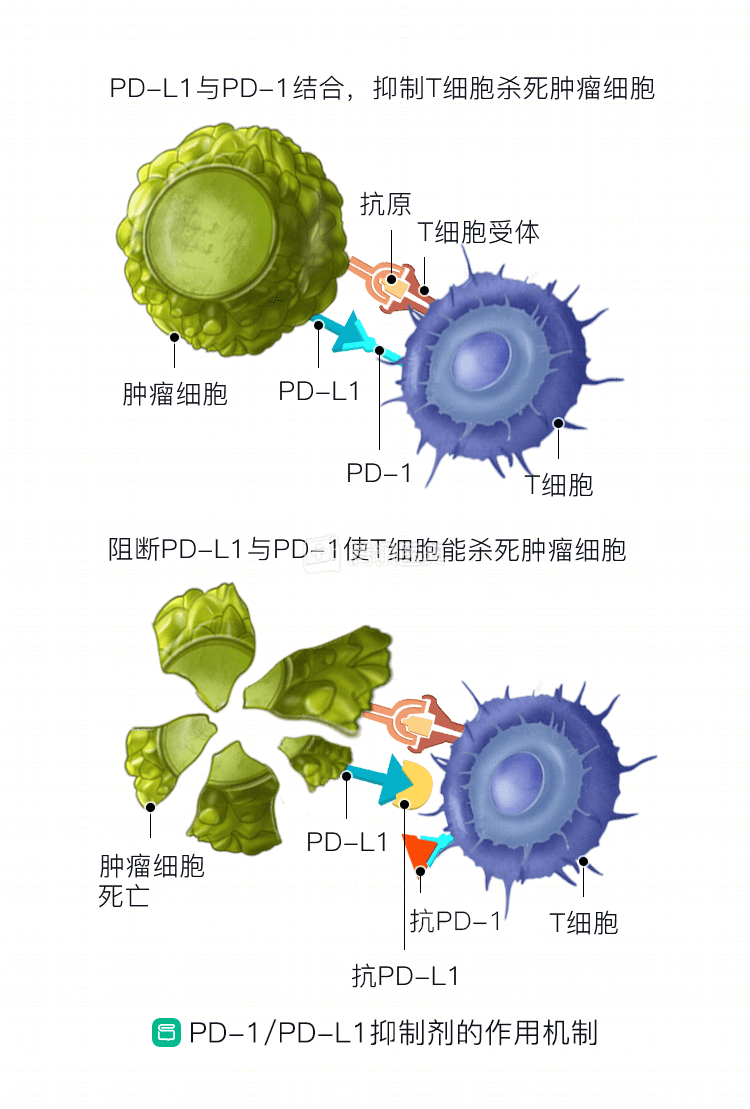
Some cancer cells express PD-L1 on their surface, which binds to PD-1 on the surface of T lymphocytes and initiates the lymphocyte “inactivation” process like a key to a lock. The lymphocytes are one of the body’s main anti-tumor force, they “do not act”, the tumor will grow up quickly. “PD-1/PD-L1 inhibitors, a large class of drugs, can interrupt the chain of “key unlocking” and rejuvenate the lymphocytes. It has been found that patients with good PD-1 / PD-L1 inhibitors have higher levels of PD-L1 on the surface of tumor cells.
2. High tumor mutational load (TMB)
TMB can be understood as how many mutations are carried on the DNA of a tumor cell, usually expressed as the number of mutations per million bases. The higher its level, the better the efficacy of the PD-1 / PD-L1 inhibitor.
3. Microsatellite instability
Mutations occur during DNA replication, causing some short, repetitive DNA sequences to change in length. These DNAs are called microsatellites (MS) and are distributed throughout the genome.
Microsatellite instability is often caused by DNA mis-match repair (MMR) defects (dMMR).
What is MMR?
What is MMR? It is an important self-repair mechanism. As our cells proliferate, DNA is replicated or recombined, and this process can “go wrong” (base mismatch) and lead to a variety of diseases. The MMR accurately identifies and repairs these errors to prevent the development of disease, including cancer.
The MMR defect is a malfunctioning repair mechanism. It was found that patients with high MSI / dMMR types of solid tumors, such as colorectal, endometrial, bile duct, and gastric cancers, had an overall efficiency of about 46% with PD-1 / PD-L1 inhibitors after failure of first-line therapy.
It is important to note that these markers are not perfect in guiding immunotherapy overall and need to be further validated in the esophageal cancer field.
Immunotherapy also has adverse effects
The mechanism of immunotherapy is to mobilize the “fighting power” of T-lymphocytes to kill tumor cells. But these morale boosting T-lymphocytes can sometimes get “red-handed” and may attack their own healthy tissues or cells. Therefore, immunotherapy can have adverse effects, including:
- Colitis (less than 5%)
- Pneumonia (2 to 5%)
- Immune-related liver injury (5%)
- Dermal adverse reactions (30%)
- Thyroid abnormalities (5-10%)
- Hepatitis (1%)
- Cardiomyopathy (less than 1%)
- Neurotoxicity (less than 1%)
Most adverse reactions can be controlled with medications, but neurotoxicity, myocarditis, and hepatitis may be life-threatening.
Clinical trials found that anti-PD-1/PD-L1 monotherapy for esophageal cancer caused lethal adverse reactions that generally occurred around day 40 after treatment, with pneumonia being the most common (35%), followed by hepatitis (22%), colitis (17%), neurotoxicity (15%), and myocarditis (8%); of these, the most lethal was myocarditis, at 39.7%  ;; also be aware of the risk of esophageal perforation, all of which require monitoring and evaluation by a physician.
The combination of multiple immunotherapeutic agents is often associated with more severe adverse effects than monotherapy. Studies have found that anti-PD-1/PD-L1 monotherapy is associated with less severe adverse effects than the combination of anti-CTLA-4 as well as PD-1/PD-L1.
Co-written by:
Dr. Jianling Zou, Shanghai Tenth People’s Hospital
Dr. Jiao Xi, Peking University Cancer Hospital