What is high-energy focused ultrasound (HIFU)?
What is HIFU?
High-intensity focused ultrasound (HIFU), or “HIFU” for short, uses ultrasound waves with the advantages of large penetration depth, strong directionality, good focus, and fatty tissue hypothermia to emit hundreds of low-energy beams of ultrasound outside the body through soft tissue (also called “acoustic channels”) and focus in vivo and directly on the target tissue-tumor tissue. The HIFU is an ultrasound that is focused in vivo and acts directly on the target tissue – the tumor tissue – by emitting hundreds of beams of low-energy ultrasound through the soft tissue (also called “acoustic channels”).
But the focus only addresses one point (also called the “focal point”; HIFU can raise the temperature of the focal point in the tumor to 65-100°C in 0.25 seconds), and the point becomes the line, the line becomes the surface, and the surface becomes the body, causing coagulative necrosis of the entire tumor to achieve the goal of ablation.
HIFU is indicated for solid abdominal and pelvic tumors that are accessible by ultrasound, have adequate access to the acoustic beam, and require a tumor depth of not less than 1 cm. The HIFU has been widely used in the treatment of abdominal and pelvic solid tumors, such as pancreatic cancer, liver cancer, kidney cancer, retroperitoneal tumors, uterine fibroids, ovarian cancer, prostate cancer, metastatic tumors in the abdominal and pelvic cavities, breast cancer, and osteosarcoma, with more widespread use in pancreatic cancer, retroperitoneal tumors, and uterine fibroids.
But because of the physical properties and focusing principle of ultrasound, tumors in the following organs or sites should not be treated with HIFU:
- If there are scars, gas-containing tissues (e.g., bowel), pubic bone, intracavitary birth control ring, venous embolism, arterial wall calcification, etc., on the ultrasound channel;
- The built-in probe of the HIFU device does not clearly visualize the tumor;
- Tumors of air-containing cavity organs, such as lung cancer and intestinal cancer;
- Tumors of the central nervous system;
- Tumors of the central nervous system
- Tumors that are less than 1 cm from the epidermis or have infiltrated the epidermis;
- Tumors of the central nervous system;
- HIFU localized skin infection or radiation of 45Gy or more;
- Patients with major organ insufficiency;
- Patients with coagulation disorders.
What are the applications of HIFU in prostate cancer?
HIFU treats prostate cancer in two main ways:
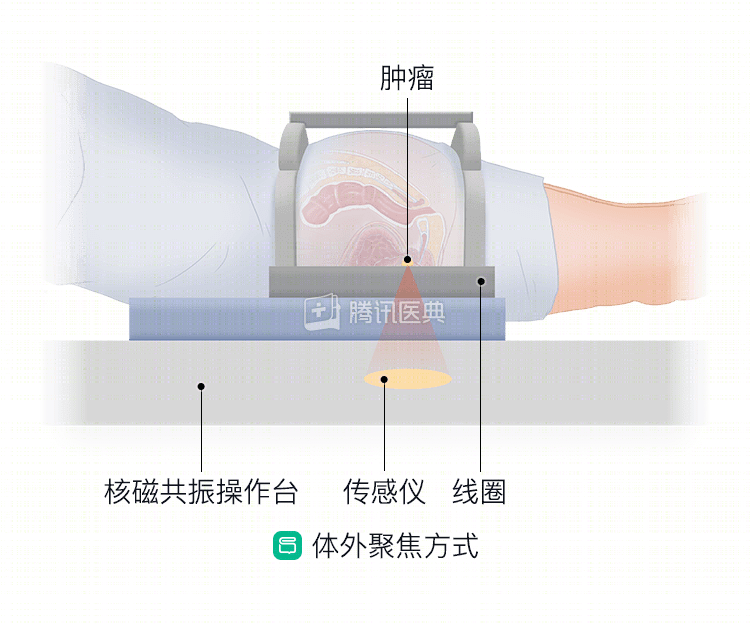
- Ex vivo focused modality: does not require any anesthesia and requires several treatments;
- In vivo focusing modality: performed under general anesthesia or lumbar anesthesia and treats prostate cancer via the rectum.
Scope of treatment
- Selective Focused Therapy: Treatment of the tumor and some of its adjacent prostate tissue based on imaging localization, but because prostate cancer often exhibits multicentric growth, when a tumor occurs on one side, there may also be microscopic lesions on the other side that are indistinguishable on imaging. Therefore, there is an increased chance of residual tumor in the prostate after treatment;
- Expanded focused therapy: i.e., treatment of the entire prostate gland. The disadvantage is that it is likely to cause postoperative sexual dysfunction, but the probability of residual tumor is greatly reduced, and because most patients are elderly and have lost most of their sexual function before HIFU, expanded focused therapy is mostly advocated.
The clinical use of HIFU in prostate cancer treatment is currently divided into HIFU alone and HIFU combined with other treatments. The HIFU-related treatments are selected individually according to the indications and for patients with different conditions, which can fully utilize HIFU and achieve the best treatment effect.
HIFU alone
Primarily for patients with localized early-stage prostate cancer, meeting the following indications:
- Age >70 years;
- Gleason score ≤7;
- PSA ≤ 15 μg /L;
- Refusal of surgery or unsuitable for surgery due to complications;
- TNM staging T1-2 NX-0 M0.
HIFU combined with other treatment options
- HIFU in combination with transurethral resection of the prostate
Prostate cancer is mainly found in the peripheral zone of the prostate, and when the tumor size exceeds 50 mm, the limitation of the transducer focal length often leads to the inability of the ultrasound focus to reach the peripheral lesion, limiting the use of HIFU in localized early prostate cancer. The results of this study are very promising.
- HIFU in combination with endocrine therapy
Endocrine therapy is widely used in prostate cancer, but during endocrine therapy, prostate cancer may eventually progress to desmoresistant prostate cancer, resulting in insensitivity to endocrine therapy. The current clinical use of endocrine therapy in combination with HIFU has shown more satisfactory therapeutic results. Shrinking the tumor to within the treatable range of HIFU by endocrine therapy offers a new therapeutic opportunity for some prostate cancer patients.
But the treatment tends to lead to conversion of prostate cancer to hormone-non-dependent.
- HIFU in combination with radiation therapy
Radiation therapy for prostate cancer consists of 3 main modalities: intertissue radiation therapy, external radiation therapy, and 3-dimensional conformal radiation therapy. However, prostate cancer is mainly multicentric growth and has a high recurrence rate after radiotherapy, so the effect of radiation therapy on prostate cancer is unsatisfactory.
Currently, combining HIFU with radiation therapy to suppress prostate cancer has shown satisfactory therapeutic effects with two main mechanisms:
- Radiotherapy inhibits tumor DNA synthesis and kills tumor cells directly, but some cells become oxygen-depleted, leading to tolerance to radiotherapy. HIFU can increase the oxygen content of this part of cells, which inhibits the tolerance to radiotherapy and prevents tumor damage repair, thus achieving complete killing of tumor cells;
- HIFU can activate tumor cell immunity to a certain extent to kill tumor cells.
.
Which prostate cancer patients are suitable for HIFU treatment?
HIFU has the advantages of no surgical exposure or puncture-mediated, no incision, no bleeding, no pain, no radiation, no emission line contamination, simple protection, and a high degree of safety and reliability.
HIFU is indicated for patients with the following conditions:
- Prostate cancer with clinical stage T1c~T3 and not suitable for radical prostatectomy (e.g., age >70 years, life expectancy <10 years);
- Combined with other serious diseases that prevent or refuse surgery;
- as salvage therapy for local recurrence after external radiation radiotherapy;
- As salvage therapy for local recurrence of prostate cancer after radical prostatectomy;
- As retreatment after failure of prior HIFU therapy or as palliative treatment for tumor reduction due to pain, bleeding, and dysfunction caused by excessive tumor size.
What complications can result from HIFU treatment for prostate cancer?
The main complications after HIFU treatment for prostate cancer include:
- Urinary obstruction: including bladder neck obstruction, urinary retention, and voiding dysfunction;
- Urinary incontinence;
- Urinary tract irritation: urinary frequency, urgency, and painful urination;
- Erectile dysfunction;
- Urinary tract infections;
- Urinary bleeding;
- Epididymitis;
- Other: urorectal fistula, levator muscle necrosis, cardiovascular events, etc.
Most of the above complications can be relieved and cured by conservative treatment, such as urinary tract irritation symptoms, urinary tract infection, epididymitis, mild urinary incontinence, and erectile dysfunction, but a small number of serious complications require interventions such as surgical treatment, such as urorectal fistula.
Although complications of HIFU are inevitable, some of the above complications such as erectile dysfunction, urorectal fistula, and anal raphe necrosis are mainly caused by damage to surrounding adjacent blood vessels, nerves, and other tissues due to lack of precision, thermal injury, and other factors.
Currently, HIFU is used in combination with MRI to adjust the extent of resection by monitoring the temperature of the resected portion of the HIFU and the surrounding tissue in real time by MRI temperature to improve the precision of the operation, reduce the damage to important structures (nerves, blood vessels, rectum, etc.) and overcome the shortcomings of the resected tumor.
In addition to combined MRI, the use of ultrasound contrast agents to enhance the contrast between the tumor and surrounding tissue and the use of elastography to monitor the extent of thermal damage in real time are also hot topics of research, which can effectively improve the accuracy of HIFU treatment of tumors and reduce unnecessary tissue damage.