With continued improvements in radical surgery techniques and advances in medical equipment, radical prostate cancer surgery now hopes to achieve 3 things:
- complete removal of prostate cancer to prolong patient survival;
- To avoid postoperative urinary incontinence and restore urinary control as soon as possible;
- Preserve the erectile function of the penis as much as possible.
In which, ensuring complete removal of the tumor remains the primary goal. The vast majority of patients who undergo radical surgery achieve satisfactory outcomes, but no procedure is completely risk-free, and some patients may still experience intraoperative and postoperative complications, more commonly bleeding, urinary incontinence, and postoperative erectile dysfunction.
Bleeding
When you think of surgery, you may see a lot of “sword and blood” and many patients and families are very concerned about bleeding during and after surgery, which may be true in the era of traditional open surgery.
First of all, it should be noted that most surgical procedures are basically bleeding during and after surgery, and radical prostate cancer surgery is naturally no exception, but the amount of bleeding varies relatively widely depending on the patient’s condition, the surgical approach used, the surgeon’s proficiency in the specific surgical approach and surgical experience, and many other factors.
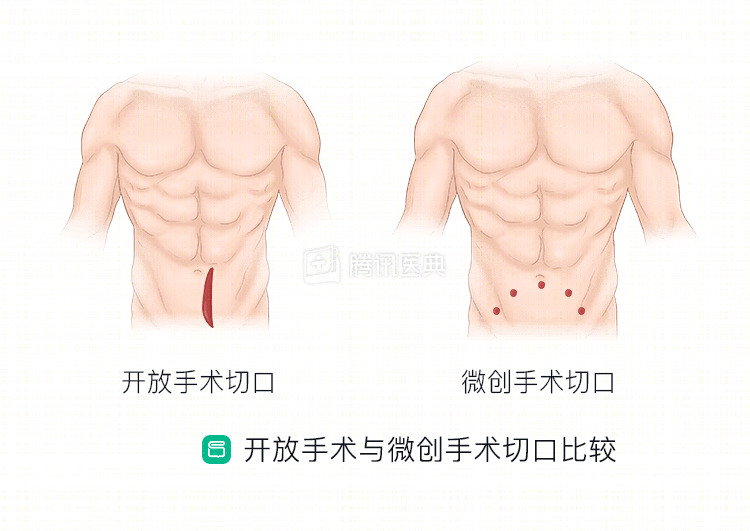
With the development of minimally invasive surgery, laparoscopic or robot-assisted laparoscopic radical prostate cancer treatment is now widely performed, and the traditional large-incision surgical approach is rarely used. In general, minimally invasive surgery has resulted in minimal patient bleeding, and some urologists have even achieved “bloodless” surgery.
We have all probably donated blood before, and a single donation of 200ml or 400ml does not have a significant impact on our health. Some people mistakenly believe that “the total amount of blood in a person is fixed and cannot be replenished or recovered after bleeding”. Moreover, the patient is under medical monitoring during the operation, and the doctor will plan to replenish the patient’s blood volume and adjust the patient’s physical condition before, during and after the operation. The patient’s blood volume and hemoglobin are normal, and even if he loses 400 ml of blood under medical monitoring, it will not have a major impact on the body.
Of course, there are a few patients who lose more blood and require blood transfusion therapy because of the large size of the prostate, the difficulty and length of the surgery, the presence of preoperative anemia, and the occurrence of secondary bleeding after surgery. We should know that blood transfusion is a normal part of surgical treatment. If the condition requires blood transfusion, it is recommended that the patient and family members actively cooperate with the doctor to do a good job of blood transfusion treatment, and there is no need to worry too much about the possible adverse effects of blood transfusion. At present, the source of blood products in regular hospitals in China has adequate quality assurance and undergoes strict testing, and the occurrence of adverse reactions to blood transfusion is still relatively rare.
Urinary incontinence
Radical prostate cancer surgery involves complete removal of the prostate gland and anastomosis of the bladder and urethra to restore continuity, and urinary incontinence is a common postoperative complication with an incidence of 5% to 40% and a significant impact on quality of life in severe cases. Urinary tract infection, urethral sphincter injury, and bladder dysfunction are the main causes of postoperative urinary incontinence.
Regular pelvic floor function training before surgery and preservation of structures such as the bladder neck, neurovascular bundle, and puboprostatic ligament as much as possible during surgery can significantly improve the patient’s postoperative urinary control function and reduce the incidence of incontinence.
If postoperative incontinence occurs, it can usually be restored with the following treatments. Common treatments include Kegel exercises, biofeedback and electrical stimulation, and medications.
- Kegel exercises (pelvic floor exercises or anal contraction exercises) are the simplest and most effective method and may be the first choice for initial treatment of mild to moderate incontinence.
- Biofeedback, which monitors the electrical activity of the pelvic floor muscles with the help of a special therapeutic instrument and translates the information about the activity into auditory and visual signals back to the patient, instructs the patient to perform correct and autonomous pelvic floor muscle training and to form a conditioned reflex, is also more widely used.
- Electrical stimulation works by stimulating nerves and muscles, inhibiting and decreasing bladder contractility by forming impulses that excite sympathetic pathways and inhibit parasympathetic pathways. Therefore, biofeedback and electrical stimulation are both often used in combination.
- Pharmacologic treatment is primarily for patients with mild urinary incontinence.
A very small number of patients who do not see significant improvement in incontinence after these treatments may be considered for surgical treatment. Common methods include artificial urethral sphincter implantation and ball urethral spongiosuspension, but again, surgery may entail some complications.
Postoperative erectile dysfunction
Radical prostate cancer surgery is complex and one of the most difficult procedures in urology. Avoiding postoperative incontinence and preserving as much erectile function as possible while ensuring complete removal of the tumor is the goal of all urologists.
The erectile function of the penis is innervated. The nerves that govern penile erection are contained in a structure called the “neurovascular bundle” on each side of the prostate, posterior and lateral. In order to remove the lesion as completely as possible, traditional radical prostate cancer surgery usually damages the “neurovascular bundle”, resulting in erectile dysfunction in most patients after surgery.
In recent years, radical prostate cancer surgery has been performed to preserve the neurovascular bundle as completely as possible while ensuring complete resection of the tumor, thus preserving sexual function as much as possible, and many patients have benefited from this postoperatively. However, some patients who have undergone surgery to preserve the neurovascular bundle still experience erectile dysfunction after surgery. This is partly due to the fact that there are more anatomical variations in the neurovascular bundle, meaning that some people have a different location of the erectile nerve than the average person and are vulnerable to intraoperative damage; on the other hand, it is also possible that the blood vessels or cavernous bodies supplying the penis were damaged during surgery.
With recent improvements in neurovascular bundle protection techniques, most patients can retain normal sexual function after surgery; specifically, three-quarters of patients typically regain normal sexual function within one year after surgery.
Related reading: