With the advancement of medical technology and equipment, the treatment of prostate cancer is changing rapidly and there are many different kinds of treatment methods, such as injection, medicine, testicle cutting, radical surgery, radiotherapy, etc. It seems that each treatment method is very effective, so how should you choose?
The general principle of treatment for prostate cancer is “individualized treatment on a case-by-case basis” and the common treatment options can be broadly classified as follows:
Wait and see
Some patients with a clear diagnosis of prostate cancer are unwilling or too weak to undergo active treatment, but instead are closely monitored and followed until symptoms appear and then some palliative treatment is given to relieve the symptoms of metastatic lesions. This is a conservative approach to treating prostate cancer and is only indicated for the following conditions:
- Patients with advanced disease with distant metastases (e.g., bone metastases) have a strong personal desire to avoid adverse effects due to treatment and have far greater concerns about the risks and complications that accompany treatment than the expectation of prolonged survival and improved quality of life.
- Some patients have a life expectancy of less than 5 years and refuse to accept the potential adverse effects of active treatment despite adequate information. Therefore, wait-and-see therapy is not used in principle unless the patient himself is strongly opposed to active treatment or for other reasons.
Active monitoring
Unlike wait-and-see, active surveillance is for patients at low clinical risk with a chance of radical treatment. Such patients are fully aware of and accept the risk of local tumor progression and metastasis and do not proceed to active treatment immediately because of concerns about quality of life, surgical risks, etc., choosing instead to follow closely, actively monitor disease progression, and treat the tumor when it progresses to an acceptable level that they have predetermined.
In general, active surveillance is only appropriate for:
- Very low-risk prostate cancer (PSA values between 4 and 10 ng/m1, Gleason score less than 6, positive biopsy index less than 3, less than 50% tumor per puncture specimen, clinical stage less than T2a).
- Clinical stage T1a, well or moderately differentiated tumor cells in relatively young patients with prostate cancer and a life expectancy greater than 10 years.
- Clinical stage T1b to T2b, asymptomatic patients with well-differentiated or intermediate tumor cells and a life expectancy of less than 10 years.
Patients need to be followed closely with PSA, transrectal prostate ultrasound, and prostate puncture biopsy during the course of active surveillance. Once disease has progressed, aggressive treatment is required. For patients with low-risk limited prostate cancer with a life expectancy greater than 10 years, radical prostatectomy is preferred, followed by radical radiotherapy, with some patients strongly requesting or willing to actively participate in relevant clinical trials, and active surveillance is generally not recommended.
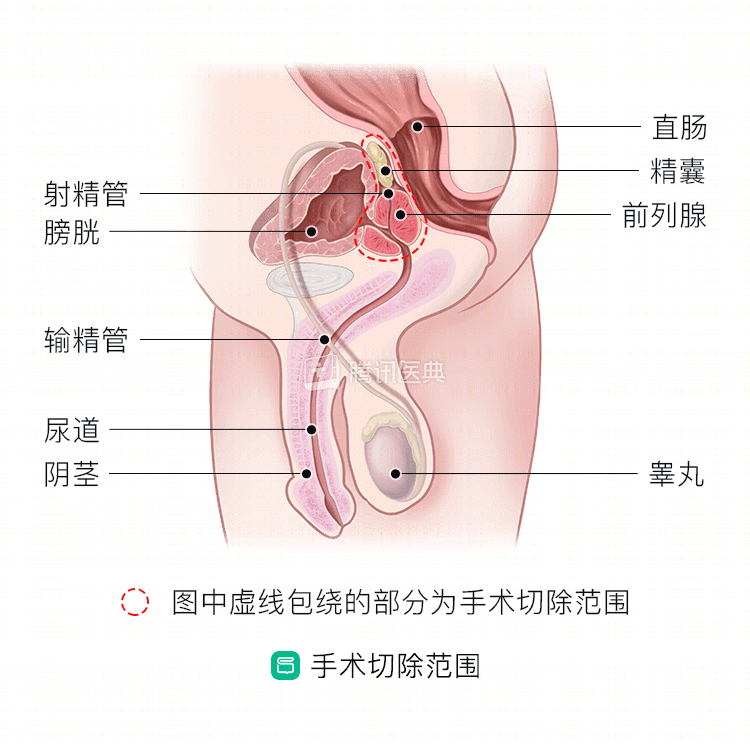
Radical surgical treatment of prostate cancer
Radical prostatectomy or radical prostatectomy, as it is often called, is the most effective way to treat patients with early and some intermediate stage prostate cancer to achieve a cure. It includes traditional open surgery, laparoscopic, and robotic-assisted laparoscopic radical prostatectomy.
Radical prostate cancer surgery can be considered for patients with early and some intermediate stage prostate cancer who have a life expectancy of >10 years, are in good health, do not have severe heart, lung, or brain disease, and can tolerate surgery.
- Radical surgery is recommended for patients with tumor stage T1 to T2c;
- Patients with stage T3a or high-risk limited prostate cancer (Gleason score greater than 8 or PSA greater than 20) also require adjuvant endocrine therapy or adjuvant radiotherapy after surgery;
- Patients with stage T3b to T4 can also undergo radical surgery and adjuvant combination therapy after rigorous screening.
Currently, many authors believe that radical surgery and adjuvant therapy in patients with partial regional lymph node metastases or even oligometastases can improve quality of life and benefit overall survival. However, the decision to perform surgery depends on a number of factors, including the stage of the tumor, the overall condition of the patient, the local medical level, and the clinical experience of the attending surgeon.
External radiation therapy for prostate cancer
This is commonly referred to as “radiation therapy. The treatment is divided into radical radiotherapy, postoperative adjuvant radiotherapy, postoperative salvage radiotherapy, and palliative radiotherapy for metastatic prostate cancer, which is suitable for almost all stages of prostate cancer. It is mainly used for the treatment of early-stage prostate cancer that is not amenable to surgery as well as for patients with advanced stages.
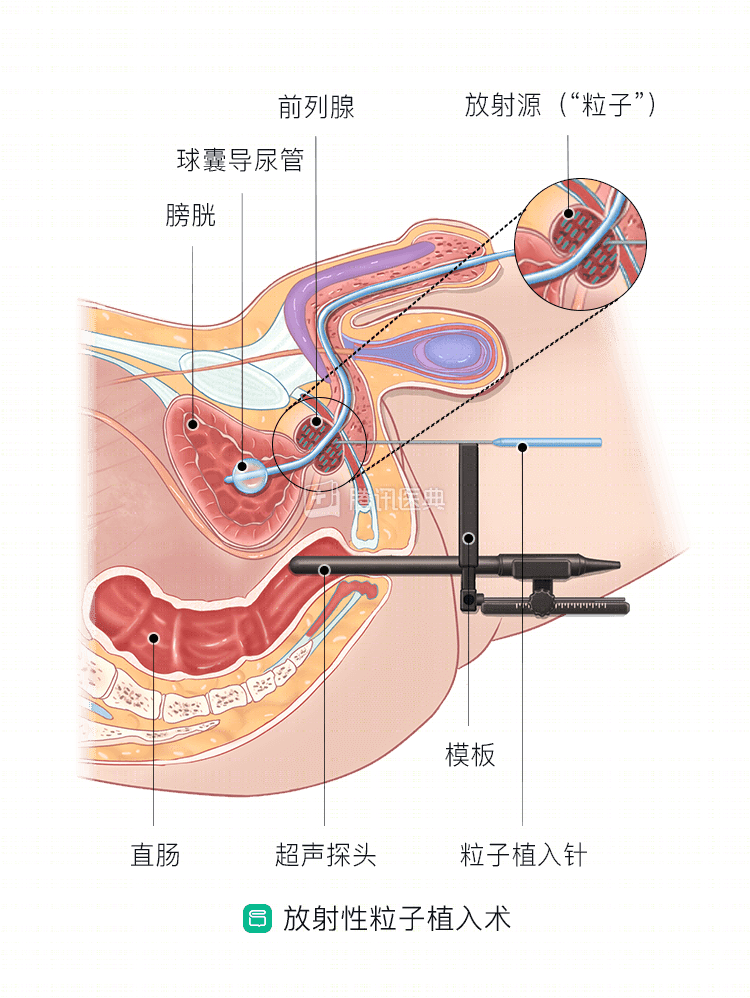
Prostate cancer brachytherapy
This is where radioactive particles are implanted into the prostate gland to kill tumor cells. Brachytherapy is primarily indicated for early, less malignant patients with a PSA of less than 10ng/ml, especially in older patients who cannot tolerate radical prostate cancer surgery; some patients may even be able to achieve radical surgery; some patients with intermediate to advanced disease may also be considered for brachytherapy combined with external radiation therapy; see your specialist for details.
Endocrine therapy for prostate cancer
Because prostate cancer cells depend on androgens as “nutrients” for growth, endocrine therapy was developed to control tumor progression if androgens are reduced in the patient’s body.
Endocrine therapy includes both depot therapy and androgen blockade therapy. In addition, the patient’s testicles are removed from the testes, and the patient’s testicles are removed from the testes. The most common method used in clinical practice is denervation plus anti-androgen drugs to maximize androgen blockade, so-called “all-androgen blockade”, which is the most effective endocrine therapy for most patients.
Endocrine therapy is widely used, usually for:
- Advanced metastatic prostate;
- Early to mid-stage prostate cancer that cannot be treated with radical surgery or radiotherapy for various reasons;
- Neoadjuvant therapy prior to radical treatment;
- Local recurrence or distant metastasis after radical treatment;
- Treatment of patients with destructive resistant prostate cancer.
Other experimental local treatments
Including cryotherapy, high-energy focused ultrasound therapy, and radiofrequency ablation of intra-tissue tumors. The decision to perform these methods depends on what is available at the local hospital in conjunction with the patient’s condition.
Of course, we reiterate here that the condition is always changing and the final treatment plan needs to be determined on a case-by-case basis by the treating physician, as only the physician knows the patient’s individual condition best. Long-term medical practice has shown that different treatments must be chosen for individual patients, otherwise it is not only difficult to achieve satisfactory results, but may even delay the timing of treatment.
In recent years, the MDT (multidisciplinary clinical team) model has quietly emerged in many developed countries and regions, representing an international trend in the treatment of malignant tumors, and a few large teaching hospitals in China, including Wuhan Tongji Hospital, are exploring the MDT model for prostate cancer. The MDT model is a multidisciplinary approach that combines the advantages and disadvantages of each patient’s specific condition to make the best treatment plan that is scientific, rational and standardized.
Related reading: