
Patients with breast cancer who receive neoadjuvant therapy prior to surgery can often directly observe changes in tumor size before and after treatment. Because tumors may change morphologically and histologically after treatment, pathologic evaluation of breast specimens before and after neoadjuvant therapy is important not only to determine efficacy and provide a basis for treatment, but also to more accurately assess the ultimate outcome of breast cancer patients.
How can pathology be performed before and after neoadjuvant therapy?
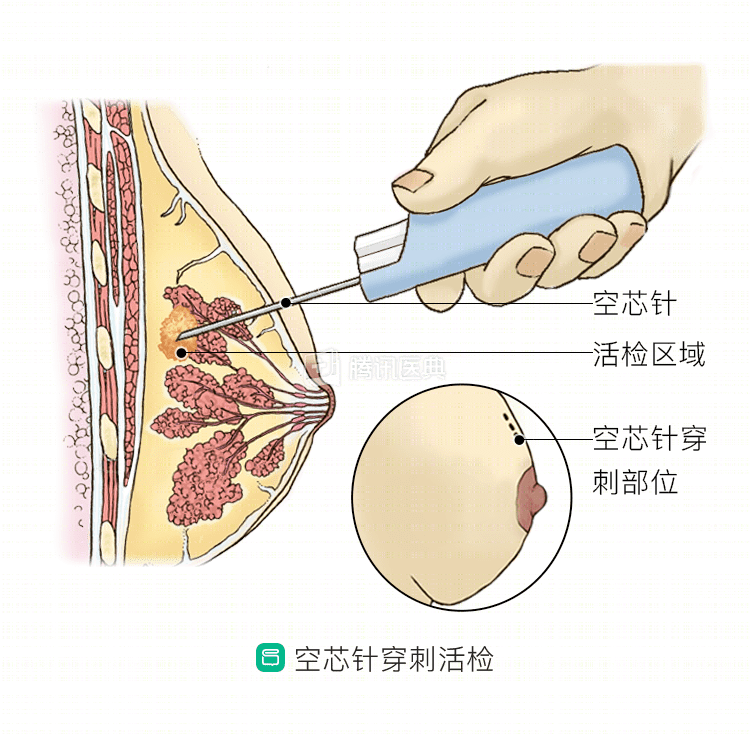
- Before neoadjuvant therapy, physicians typically use a puncture biopsy to obtain tissue specimens for pathologic diagnosis. A puncture biopsy usually provides a safe and accurate way to obtain a sufficient amount of breast tissue for a correct pathologic diagnosis and immunohistochemical testing to determine the molecular type of the tumor, which is used to guide the choice of treatment.
- After 2 to 4 courses of neoadjuvant therapy, the physician will usually evaluate the effectiveness of treatment by examination and imaging. If the evaluation reveals that the treatment is not effective, a puncture is usually performed to obtain sufficient tissue from the lesion for pathologic evaluation, which is used as a basis to modify the neoadjuvant treatment plan or to consider surgical treatment, after which a final pathologic outcome determination is made.
What pathology is checked before and after neoadjuvant therapy?
Pathologic indicators continue to be important in assessing neoadjuvant breast cancer treatment and final disease outcome, including tumor size, margin status, lymph node status, histologic staging, and vascular and lymphovascular invasion. Physicians also examine expression of estrogen receptor (ER), progesterone receptor (PR), and Human Epidermalgrowth Factor Receptor-2 (HER-2) to determine the molecular staging of the tumor, which is used to guide the selection of treatment options and predict disease outcome.
How are pathology results viewed?
The expression of some markers in tumors before and after neoadjuvant therapy is usually consistent, but because most pre-neoadjuvant testing uses breast puncture biopsies with limited sampling, when there is heterogeneity in tumor marker expression (i.e., multiple genotypes or subtypes can exist in different cells of the same tumor), this may lead to differences in the results before and after neoadjuvant therapy.
Neoadjuvant therapy itself can also alter some test results, and endocrine therapy may lead to changes in hormone receptor status, as well as changes in HER-2 expression status after trastuzumab treatment.
For these reasons, physicians will typically retest ER, PR, HER-2, and Ki-67 status if ER, PR, and HER-2 tests are negative before neoadjuvant therapy and invasive cancer remains after neoadjuvant therapy.
After neoadjuvant therapy, about 3% to 30% of patients achieve pathologic complete remission (pCR), which is the complete disappearance of tumor in the breast and regional lymph nodes when viewed microscopically. Those who achieve pCR after neoadjuvant therapy have a longer survival than those who do not achieve pCR in the same treatment cycle. When this group of patients is evaluated for pathological examination, etc., the possibility of examination failure is likely to occur due to the complete disappearance of the primary lesion and the enlarged lymph nodes in the axilla. It is important for the patient to fully understand and cooperate with the physician at this time so that the physician can accurately locate the primary lesion based on the physical examination and imaging assessment prior to neoadjuvant therapy and provide a basis for the subsequent surgical plan.
With the rapid development of molecular biology techniques, pathological examination has increasingly important applications in the selection of individualized treatment plans and prognosis prediction for breast cancer patients. Patients should also pay attention to pathological examination before and after neoadjuvant therapy and actively cooperate with their doctors to complete the examination.