Everolimus was approved by the FDA in 2009 for the treatment of kidney cancer. in 2012, everolimus was given an indication for breast cancer in Europe and the United States: in postmenopausal patients with advanced hormone receptor-positive breast cancer, when traditional endocrine drugs such as anastrozole and letrozole have failed, everolimus can be used in combination with Exemestane (Exemestane) regimen to continue treatment.
Although everolimus is available in China, it has not yet been given an indication for breast cancer. In the Chinese Society of Clinical Oncology (CSCO) guidelines for the management of breast cancer published in 2018, everolimus is recommended for some hormone receptor-positive advanced breast cancers.
In this article, we take a look at the role of everolimus, an “old” drug, in the treatment of breast cancer.
Why does everolimus work against cancer?
Why does everolimus work?
Malignant tumorigenesis is associated with a signaling pathway called “phosphatidylinositol-3- kinase/protein kinase B/mammalian target of rapamycin (PI3K/Akt/mTOR),” a “messaging pathway” that is involved in cell proliferation, angiogenesis, and other activities. This “information pathway” plays an important role in cell proliferation, angiogenesis, etc.
Aberrant activation of the PI3K signaling pathway is associated with the development, progression, and drug resistance of many solid tumors. Abnormal activation of the PI3K/Akt/mTOR pathway is frequently detected in breast cancer patients.
Everolimus is an mTOR inhibitor that inhibits abnormal activation of these pathways and exerts anti-tumor effects. In addition, for breast cancers that overexpress estrogen receptors, everolimus can also inhibit key enzymes downstream of the estrogen receptor pathway, thus exerting an antitumor effect. These are the two main pathways of everolimus against breast cancer.
The PI3K/Akt/mTOR pathway is also thought to be associated with resistance to endocrine therapy and anti-HER2 therapy in breast cancer. Therefore, theoretically, blocking this pathway could reduce the incidence of drug resistance. Therefore, everolimus may be considered for use in breast cancer patients who are resistant to endocrine therapy. 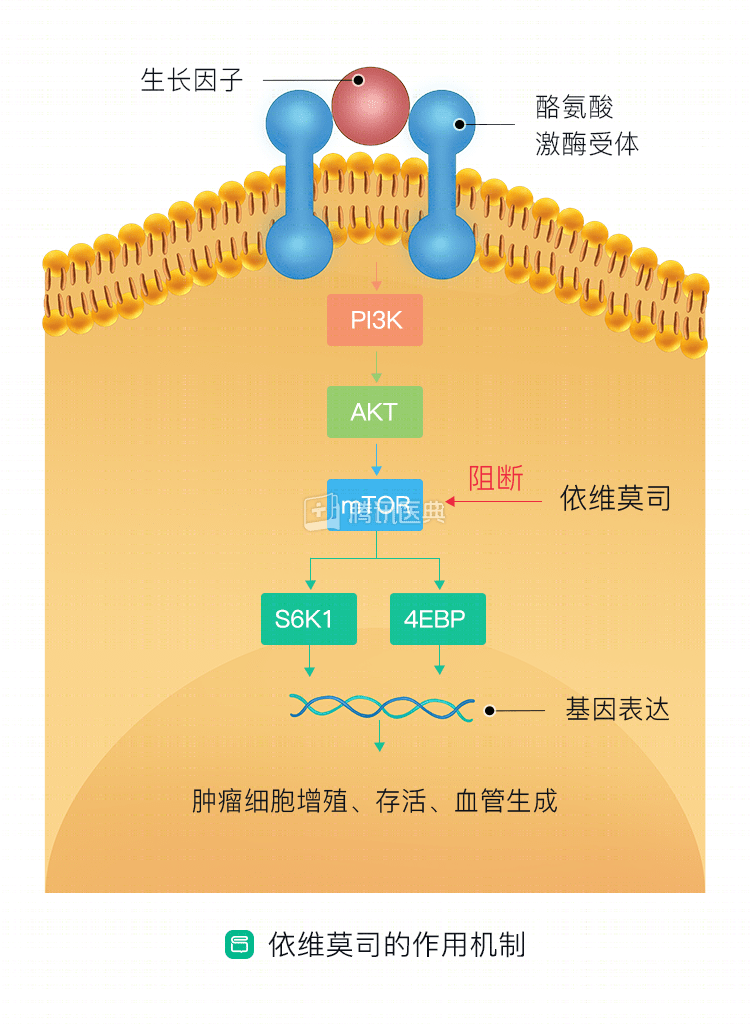
Everolimus has moved into the breast cancer endocrine therapy space
The BOLERO-2 study is a global, multicenter, phase III clinical study enrolling 724 patients with hormone receptor-positive advanced postmenopausal breast cancer who were previously treated with letrozole or anastrozole and whose disease had recurred or progressed after failure.
As a result, the exemestane combined with everolimus regimen resulted in an extended duration of tumor maintenance and stability 6.5 months, but with a slightly increased incidence of corresponding adverse events. The major side effects of the addition of everolimus included stomatitis (8%), anemia (5%), dyspnea (4%), and hyperglycemia (4%).
The BOLERO-2 study helped to make everolimus a successful entry into breast cancer treatment, making it the first mTOR inhibitor approved by the FDA for hormone receptor-positive breast cancer. The National Comprehensive Cancer Network (NCCN) and the Chinese Society of Clinical Oncology have also recommended in their guidelines that the combination of everolimus and exemestane can be used in advanced breast cancer that has failed treatment with nonsteroidal aromatase inhibitors.
In addition, endocrine agents mentioned in the NCCN guidelines that can be used in combination with everolimus include tamoxifen and fulvestrant.
‘Small gains’ in treating HER2-positive advanced breast cancer
With drug resistance in HER2-positive advanced breast cancer, the treatment options are limited. In response to this problem, researchers conducted a clinical study called BOLERO-3 to try everolimus in patients with advanced HER2-positive breast cancer who had failed anti-HER2 therapy.
Adding everolimus to vincristine in combination with trastuzumab treatment prolonged disease control by approximately 1.2 months. Common moderate adverse reactions during treatment include neutropenia, leukopenia, anemia, and stomatitis. It should be noted that the addition of everolimus treatment nearly doubled the incidence of serious adverse reactions in patients, from 20% to 42%.
Also for HER2-positive advanced breast cancer, the BOLERO-1 study used everolimus in first-line therapy in combination with trastuzumab and paclitaxel, which did not result in a significant improvement in patient survival.
Evimoxib in China
The BOLERO-1, BOLERO-2, and BOLERO-3 studies all involved Chinese patients, and their results are informative for breast cancer patients in China. The breast cancer treatment guidelines published by the Chinese Society of Clinical Oncology mention everolimus for the treatment of postmenopausal hormone receptor-positive advanced breast cancer: in combination with a steroidal aromatase inhibitor after failure of nonsteroidal endocrine therapy.
A phase II clinical study (No. CTR20170589) is currently underway in our population, according to the China Drug Clinical Trials Registration and Information Disclosure Platform.
The study is planned to enroll 160 menopausal patients with estrogen receptor-positive, HER2-negative advanced breast cancer to evaluate the efficacy and safety of everolimus in combination with exemestane in Chinese patients.
Summary
For patients with advanced postmenopausal breast cancer who are hormone receptor positive and HER2 negative, if endocrine therapy fails, everolimus might be considered when appropriate to further delay tumor progression. Of course, participation in clinical studies is also an important way to gain access to treatment.
Taking the available evidence together, the increased use of everolimus in HER2-positive advanced breast cancer after resistance to anti-HER2-targeted therapy may be an option. The place of everolimus in the first-line treatment of HER2-positive advanced breast cancer will have to be further clarified.