1. Age
The incidence of prostate cancer increases dramatically with age. Although the disease is very rare in men under age 50, the incidence increases exponentially thereafter.
An epidemiological statistical survey conducted in England and Wales in 1992 showed that the incidence of prostate cancer in men increased significantly with age:
- 50 to 56 years of age: 8 per 1,000
- 60 to 64 years: 68 per 1,000
- 70 to 74 years old: 260 per 1,000
- 75 to 79 years old: 406‰
2. Family history of disease
About 15% of men diagnosed with prostate cancer have a first-degree male relative (e.g., brother, father) with prostate cancer, compared with about 8% in the US population.
About 9% of prostate cancers may be caused by a genetic susceptibility gene.
Some researchers have conducted disease-associated genetic analyses and found a rare autosomal gene that may cause cancer in some families, but the body of evidence available suggests that the genetic mechanism of prostate cancer may be quite complex.
3. Hormone levels
The development of the prostate is dependent on the secretion of dihydrotestosterone (DHT) by the testes during fetal life. Testosterone is produced by the action of 5-alpha reductase to produce dihydrotestosterone, which then causes masculinization of the mesonephric tubular structures and development of the internal gonads. The affinity of dihydrotestosterone for androgen receptors is 4 to 50 times greater than that of testosterone, and it is dihydrotestosterone that promotes normal prostate development.
Other evidence that cumulative prostate exposure to androgens is associated with an increased risk of prostate cancer supports this conclusion, including:
- Benign prostatic hyperplasia and prostate cancer do not occur in men who are deprogrammed before puberty.
- Almost all forms of androgen deficiency lead to prostate degeneration, decreased levels of prostate-specific antigen (PSA), apoptosis of prostate cancer cells and epithelial cells, and response to therapy (anti-androgen therapy) in patients with prostate cancer.
- Results from two large preventive chemotherapy trials using 5-alpha reductase inhibitors (finasteride and dutasteride) suggest that androgen levels in the prostate affect the risk of prostate cancer. In both studies, the overall risk of prostate cancer was reduced, yet the risk of high-grade prostate cancer was increased.
4. Race
The risk of prostate cancer incidence and death was higher in blacks, intermediate in whites, and lowest in the Japanese population. There are conflicting data on the etiology of these outcomes, but there is research evidence that the level of health care may have some impact on clinical outcomes for patients.
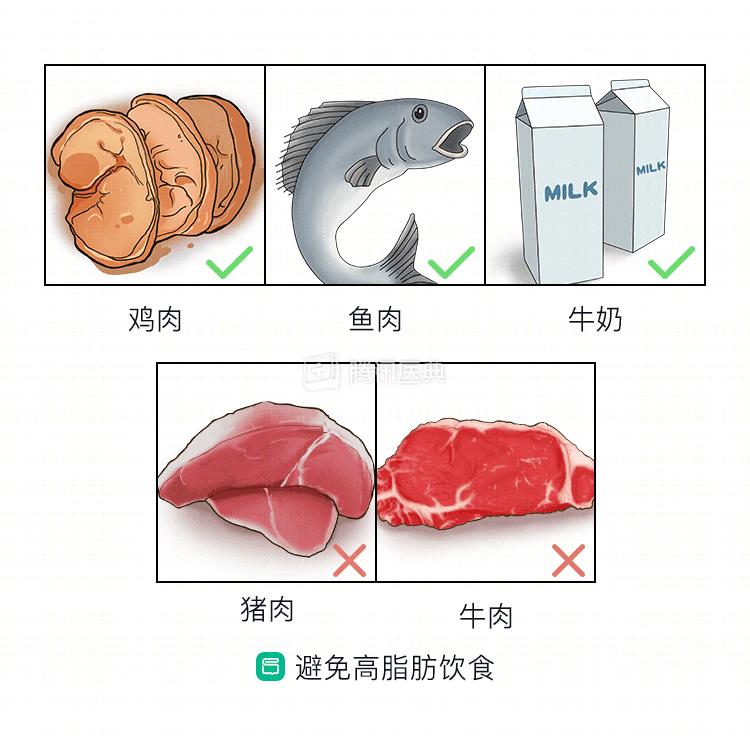
5. Dietary fat
Interestingly, the results of an observational study showed that although the incidence of underlying (occult, histologically altered) prostate cancer is similar worldwide, the true clinical incidence varies from country to country and can even vary up to 20-fold.
Previous studies have demonstrated a direct relationship between prostate cancer-related mortality in a country and the total calories from fat consumed per capita in that country. Studies of the Japanese population have shown that native Japanese have the lowest risk of clinical prostate cancer, with the first generation of Japanese Americans having a moderate risk and subsequent generations of Japanese Americans already having a risk comparable to that of Americans.
Studies in animal models of prostate cancer have shown lower tumor growth rates in the low-fat diet group. Many case-control studies have shown a correlation between dietary fat content and prostate cancer risk, but such studies have not reached a uniform conclusion.
Fats of animal origin appear to be most strongly associated with an increased risk of prostate cancer. The decline in cancer mortality announced in the United States in 1996 is likely due to a reduction in dietary fat intake in the US population during this period.
The reason for the association between prostate cancer and dietary fat is unclear. So far, researchers have proposed the following hypotheses:
- Dietary fat may increase serum androgen levels, thereby increasing the risk of prostate cancer.
- Some types of fatty acids, or their metabolites, may induce prostate cancer or promote the progression of prostate cancer.
In addition, an animal model trial showed that a high-fat diet during pregnancy in rats led to a significantly higher chance of prostate cancer in their male offspring.
6. Dairy products and calcium
A meta-analysis of 10 cohort studies (8 from the United States and 2 from Europe) showed an 11% increased risk of prostate cancer in the highest dairy intake group compared with the lowest dairy intake group and a 39% increased risk of prostate cancer in the highest calcium intake group compared with the lowest calcium intake group. In addition, the risk of advanced prostate cancer was increased by 33% and 46% in the highest dairy and calcium intake groups, respectively, compared with the lowest group.
Therefore, higher intake of dairy products and calcium may increase the risk of developing prostate cancer, although to a lesser extent.
7. Multivitamins
A large study that included nearly 300,000 men showed no association between regular multivitamin use and the risk of early or limited prostate cancer; however, men who overdosed on multivitamins had a significantly increased risk of advanced and fatal prostate cancer.
8. Folic acid
A randomized, placebo-controlled clinical trial conducted from 1994 to 2006 was designed to investigate whether aspirin/folic acid could prevent colorectal cancer. The results found that taking 1 mg of folic acid supplements daily increased the risk of prostate cancer.
However, in people not taking the multivitamin, higher levels of folic acid in the diet and blood appeared to help reduce the risk of prostate cancer.
The above results suggest that folic acid may play a very complex role in the development of prostate cancer.
9. Cadmium exposure
Cadmium exposure may be associated with occupational exposure occurring during the production of nickel-cadmium batteries or during smelting in cadmium recycling plants, and may also be associated with inhalation of cigarette smoke.
Early studies suggested a clear association between cadmium exposure and prostate cancer risk, but some well-designed clinical trials did not find an association.
10. Dioxin exposure
Dioxin (tetrachlorodibenzo-p-dioxin,TCDD) is a herbicide contaminant that is similar to many of the components found in agricultural herbicides.
However, the National Academy of Sciences Institute of Medicine published a review of previously published studies on the relationship between dioxin and prostate cancer risk, with the final analysis concluding that the relationship between dioxin exposure and prostate cancer The relationship is inconclusive.