Tracheoesophageal fistula is a more serious complication of esophageal cancer treatment, mainly manifested by coughing up material including sputum and digestive juices, and is especially likely to occur during radiotherapy and chemotherapy. In addition, in advanced esophageal cancer, the uncontrolled growth of tumor can also lead to tracheoesophageal fistula. How to deal with esophageal fistula if it occurs? Let’s find out through a real case.
Mr. Che, 57, came to Peking University Cancer Hospital on July 14, 2017, with “choking on food for more than 2 months.
Gastroscopy revealed a circumferential bulging mass in the esophagus 35-40 cm from the incisors; pathological biopsy suggested a moderately differentiated squamous carcinoma. Follow-up imaging such as chest CT and PET-CT suggested that the mass was located in the lower thoracic segment of the esophagus, involving the ventral segment of the esophagus and invading the epithelium; there were lymph node metastases in the right upper esophageal tracheal groove, mediastinum and cardia. The clinical stage is stage IIIB, which is often referred to as “locally advanced esophageal cancer”.
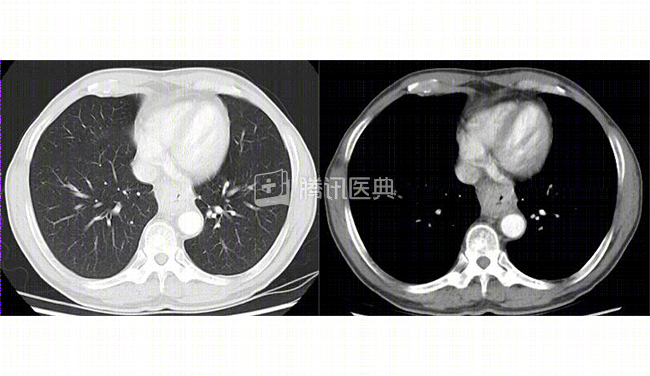
First exam (before chemotherapy)
Treatment process
After comprehensive consideration, the doctor recommended chemotherapy for Mr. Che. Because of the difficulty in eating, weight loss, and poor nutritional status at the time of the visit, he was first placed on an enteral nutrition tube for nutritional support and to improve his health.
After improvement, Mr. Che began chemotherapy with a regimen of paclitaxel + cisplatin for 21 days per cycle. Two cycles later, a repeat CT showed a smaller mass in the lower thoracic segment of the esophagus, with abnormal wall thickening of up to 22 mm, now about 15 mm, and a slightly smaller enlarged lymph node in the right tracheoesophageal groove, from 17*8 mm to 14*8 mm.
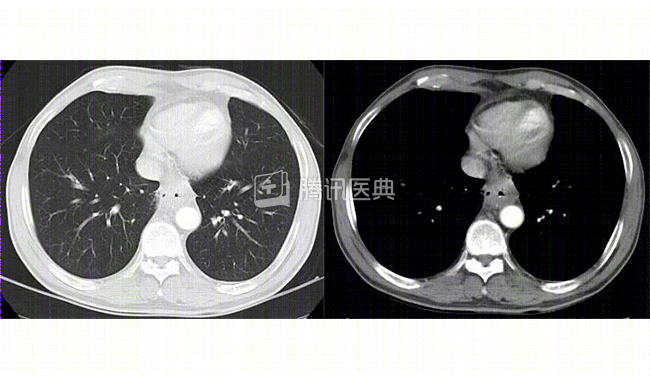
After 2 weeks of chemotherapy
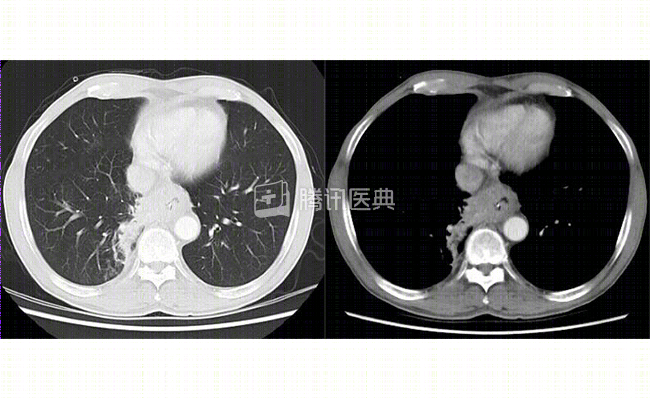
This result means that the chemotherapy is working well and that Mr. Che is improving somewhat. The doctor decided to continue with chemotherapy for a third cycle. Subsequently, a repeat CT showed a more pronounced thickening of the right wall of the lower thoracic segment of the esophagus and a new soft tissue foci in the right adjacent lung, approximately 32*22 mm, which were poorly demarcated from the lesioned esophageal wall. The patient was considered to have an esophageal mediastinal fistula with intrapulmonary inflammation.
After 3 weeks of chemotherapy
Chemotherapy for esophageal cancer, why does it cause esophageal fistula?
Doctors say:
Advanced tumors often invade the entire esophagus, and if the tumor is more sensitive to radiation or chemotherapy, it can cause the mass to rapidly regress and necrosis. The most important thing is that the tumor is not as fast as the normal tissues, so it is too late to “fill the gap”, which may lead to esophageal perforation, forming a mediastinal fistula or esophagotracheal fistula. In some advanced cases, the tumor may grow uncontrollably, causing the surface of the tumor to break down, resulting in perforation of the esophagus, which can lead to an esophageal fistula.
Simple esophageal fistula or tracheal fistula is rare. This is because the esophagus and trachea are adjacent to each other and are both lumen-like organs. If something goes wrong with the esophagus, the digestive juices from the rupture will spill into the chest cavity and the trachea will easily suffer. The pus and digestive juices may enter the trachea at any time, causing aspiration pneumonia and death by asphyxiation in severe cases, which requires prompt treatment.
Managing esophageal fistula
Mr. Che’s esophageal fistula led to a localized foci of infection in the right side of the chest, with no significant fever or chest pain, and the foci of infection were relatively limited and did not lead to widespread chest infection. The doctor decided to stop chemotherapy first, while fasting water and leaving an enteral nutrition tube for nutritional support; anti-inflammatory treatment was administered and closely monitored to prevent serious infection in the chest cavity.
The good news is that Mr. Che’s fistula was relatively small, and after aggressive treatment, the local inflammation did not further worsen, and his condition gradually stabilized, with only minor symptoms such as coughing and chest and back pain.
On March 19, 2018, Mr. Che reviewed his chest CT and found that the esophageal cancer was slightly more advanced locally than before, but was generally stable, and the chest infection was under control and not further aggravated. The doctor instructed him to come to the clinic for regular follow-up. His last visit to the clinic was on December 25, 2018. The tumor was still slowly progressing, his weight was slightly reduced, he had symptoms such as cough and chest and back pain, and his overall condition was okay. His doctor gave him symptomatic treatment for cough and pain, and continued water fasting with enteral nutritional support.
The doctor said:
If the esophageal fistula is small and the local exudate is not severe, a gastric tube is usually left in place with continuous negative pressure suction to avoid continued entry of digestive juices into the airway; it is also supplemented with anti-inflammatory therapy. In addition, nutritional support should be strengthened, because adequate nutrition is a guarantee for fistula healing. A duodenal nutrition tube (often called “nasal feeding”) is recommended for enteral nutrition to bypass the area of the esophageal fistula.
If the chest infection is severe and extensive, a gastric tube can be placed near the esophageal fistula and connected to negative pressure suction to reduce localized exudation; ultrasound or CT can be used to locate and perform closed or open drainage of the chest cavity.
If the fistula is large and the local exudate is severe, an esophageal overlay stent can be placed in the fistula site to occlude the fistula and reduce inflammatory exudate.
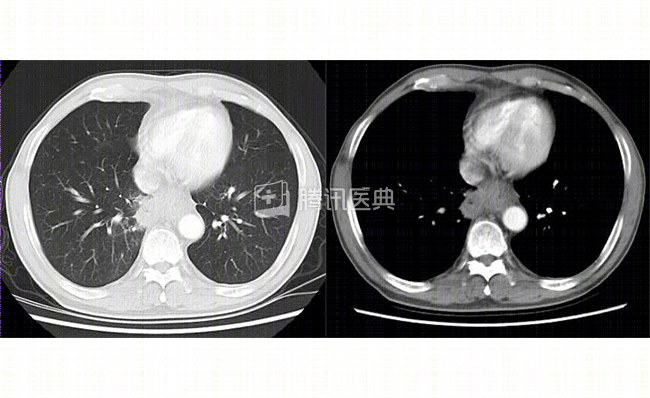
March 19, 2018 repeat chest CT: esophageal cancer slightly more locally advanced than before, chest inflammation limited
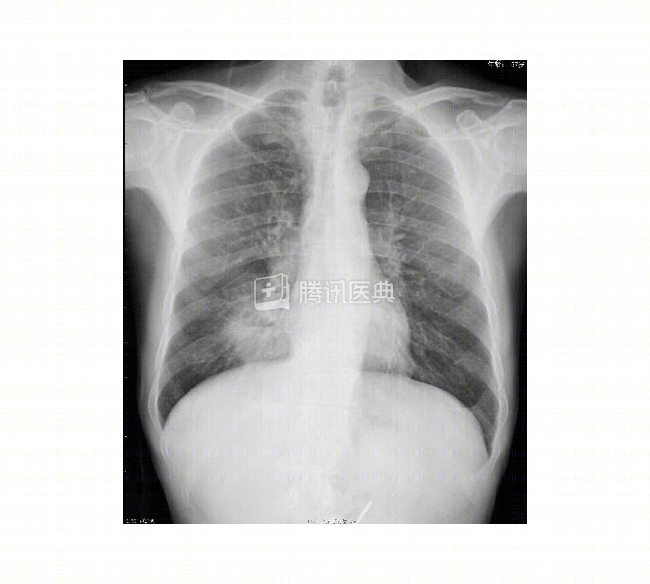
reviewed December 1, 2018, continued enteral nutrition support, patient generally doing well
Disclaimer:
Tumors are extremely complex and treatment options are highly individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from a competent physician regarding your specific treatment plan.