When you suspect esophageal cancer and go to the hospital, your doctor will often ask you to undergo some tests, such as gastroscopy and CT. Subsequently, the doctor will mark in your medical record book, the diagnosis and stage of esophageal cancer. The correct staging of the tumor is an important reminder for formulating subsequent treatment plans and judging expected treatment outcomes.
Why is it important to stage esophageal cancer?
Once esophageal cancer is diagnosed, the extent of cancer invasion should be clarified as soon as possible, which requires the collection of various stage-related test results.
Staging will help your doctor decide what additional tests are needed to make an accurate diagnosis and to develop the most appropriate treatment plan.
For example, if your clinical stage is early and there are no lymph node metastases on pathology biopsy or the risk of metastases is very low, you may be able to receive endoscopic treatment without “going under the knife.
If the tumor is in a progressive stage, your doctor may prescribe preoperative neoadjuvant therapy, which is radiation, chemotherapy, or a combination of radiation and chemotherapy before surgery, to shrink the mass and “downstage” the tumor, making it possible to remove an otherwise unresectable tumor with a higher success rate;
If the clinical stage is advanced, surgery is usually not an option, and a combination of chemotherapy and radiation therapy may be required.
How is staging done?
For staging, physicians refer to the eighth edition of “TNM Staging of Esophageal and Esophagogastric Junction Cancer,” which is the authoritative guideline published by the International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC).
Doctors typically stage esophageal cancer twice: the first time, before treatment, is clinical staging (cTNM), also known as baseline staging; the second time, done after surgery, is known as pathologic staging (pTNM) or post-surgical staging.
The physician is able to have more information through observation of intraoperative conditions and analysis of postoperative specimens. With the ability to obtain a larger amount of diseased tissue with surgery than with a gastroscopic pathology biopsy, the pathologist can be more accurate when performing the biopsy, making the final staging more accurate. The postoperative pathological staging is the main basis for doctors to judge whether the surgery was a clean cut, to estimate your treatment outcome, and to determine the next step in treatment.
In addition to these two types of staging, starting with the seventh edition of TNM staging, the concept of tumor grading (G staging) has been introduced, and G staging reflects the degree of histopathologic abnormality, or malignancy, of the tumor cells, which reflects the rate of growth and spread of the tumor . Doctors often combine G-staging with a combination of pathologic staging, your age, and general health to develop a treatment plan and to speculate on prognosis (i.e., the likely outcome or course of the disease and the chances of recovery or recurrence). Typically, a lower G-stage grade predicts a better prognosis; a higher grade predicts more rapid growth and spread, a worse prognosis, and the need for more timely and aggressive treatment.
A detailed understanding of the staging system for esophageal cancer
TNM staging – determining tumor location, size, and whether it has metastasized
The TNM staging system can display information such as the location, size and whether the tumor has metastasized, helping doctors to judge the disease, choose the right treatment method and measure the possibility of successful treatment.
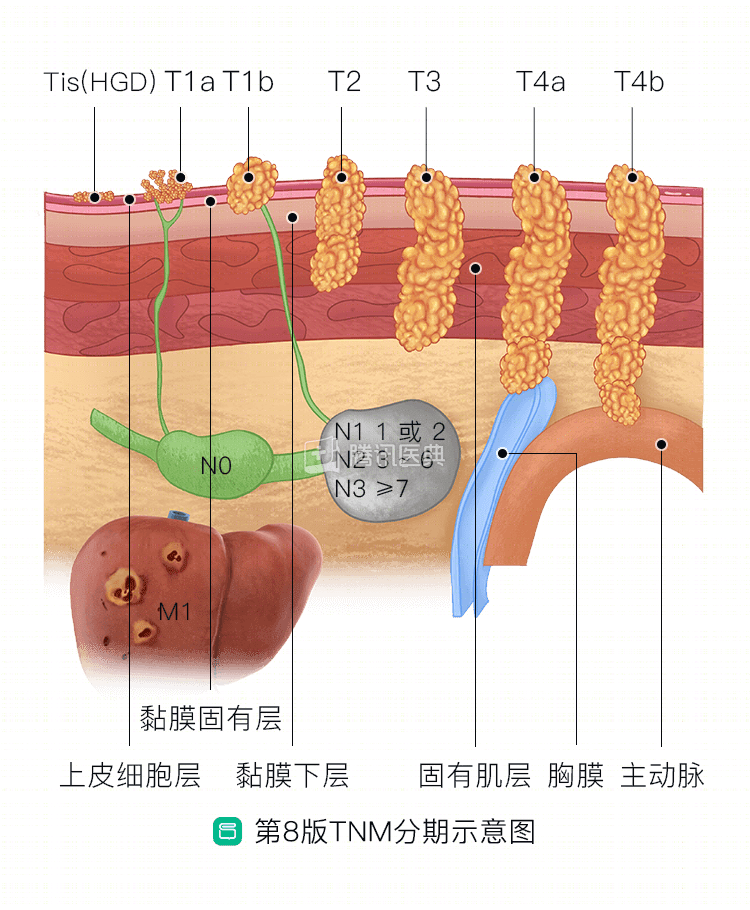
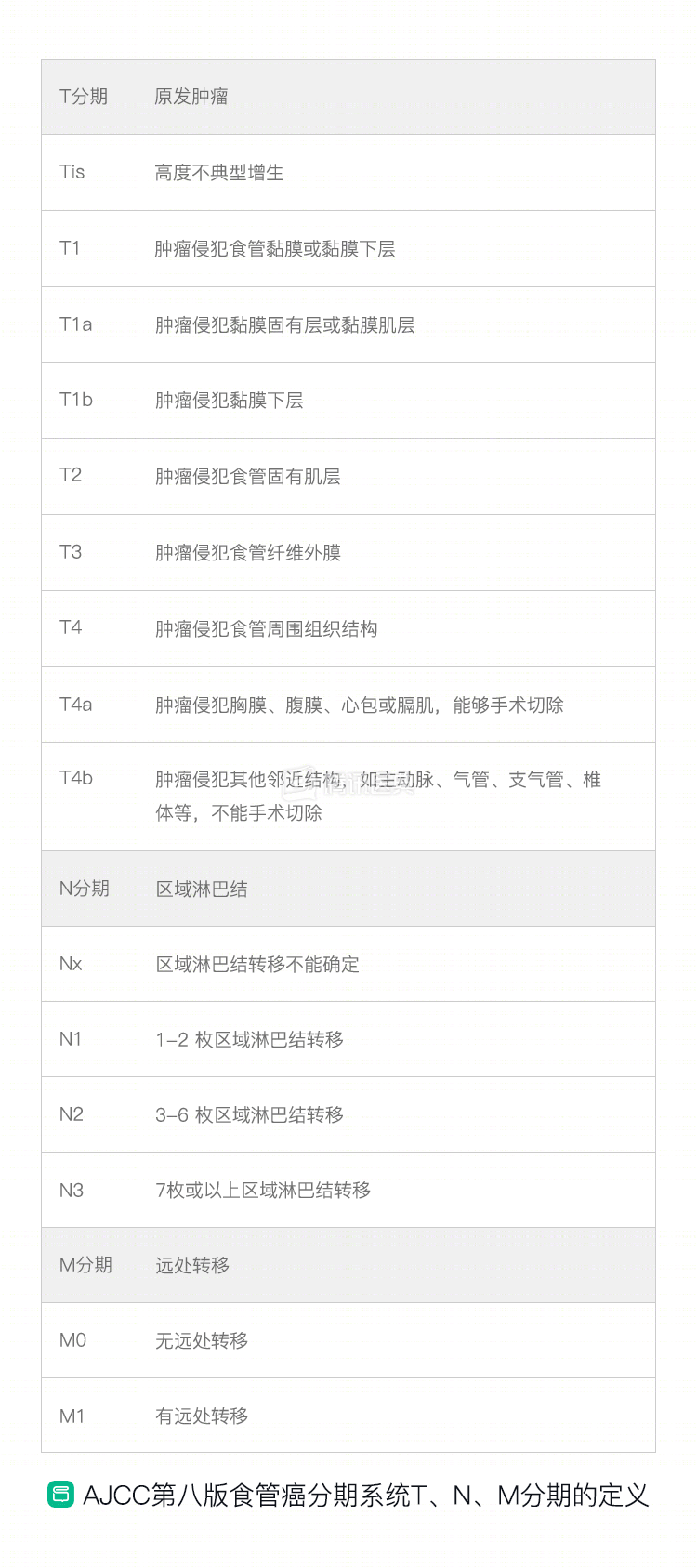
TNM staging items include primary tumor (T), regional lymph nodes (N) and distant metastases (M) (below, table below).
T (tumor), which indicates the size of the tumor and its invasion of surrounding tissue structures.
N (node), which indicates the extent of lymph node involvement and describes whether the cancer has metastasized to lymph nodes near the esophagus.
M (metastasis), indicating metastasis, describes whether the cancer has metastasized to distant sites, such as the liver, lung, bone, brain, kidney, and adrenal glands.
The pathology staging system is very complex and as a patient, it is not necessary to master it all. Clinically, physicians will classify tumors into Stages 0, I, II, III, IV based on TNM staging; each stage can be subdivided into sub-stages A and B, such as IVA and IVB, with higher stages indicating more advanced disease and worse prognosis.
G-stage – measuring the malignancy of the tumor
G staging measures the degree of differentiation, or malignancy, of the tumor (table below).
Differentiation is the process by which primitive cells change to mature cells. Depending on the degree of differentiation, it can be classified as highly differentiated, moderately differentiated, or hypodifferentiated. In general, the higher the degree of differentiation of tumor cells, the closer they are to normal cells, suggesting a lower degree of malignancy; the lower the degree of differentiation of tumor cells, the closer they are to primitive cells, suggesting a higher degree of malignancy.
For example, highly differentiated squamous carcinomas are relatively less malignant, and poorly differentiated squamous carcinomas are relatively more malignant.

To learn more about the pathological diagnosis of esophageal cancer, you can read: