Thyroid Cancer Treatment Guidelines
(2022 Edition)
I. Overview
Thyroid cancer is a malignant tumor originating from the follicular epithelium or parafollicular epithelium of the thyroid gland, and is the most common malignant tumor of the head and neck. In recent years, the incidence of thyroid cancer has increased rapidly worldwide. According to the data from the National Tumor Registry, the incidence of thyroid cancer in women in urban areas in China ranks 4th among all malignant tumors in women. The incidence of
Thyroid cancer in China will continue to grow at an annual rate of 20  . The number of thyroid cancers in China will continue to grow at a rate of 20
. The number of thyroid cancers in China will continue to grow at a rate of 20 , while PTC and FTC are collectively known as Differentiated thyroid carcinoma (DTC). Different pathological types of thyroid carcinoma differ significantly in their pathogenesis, biological behavior, histological pattern, clinical manifestations, treatment and prognosis. In general, DTC has a better prognosis; ATC is extremely malignant, with a median survival time of 7-10 months and a very poor prognosis; MTC has a prognosis in between.
(a) Surveillance screening for high-risk groups.
Screening for thyroid tumors is not recommended for the general population. However, if you have a history of the following, you are at high risk for thyroid cancer and should be screened as early as possible: 1. history of childhood head and neck radiation exposure or exposure to radioactive fallout; 2. history of systemic radiation therapy; 3. history of DTC, MTC or multiple endocrine neoplasia (MEN) type II, familial polyposis, certain Prior or family history of thyroid cancer syndromes (e.g., multiple malignancy syndrome, Carney syndrome, Werner syndrome, and Gardner syndrome).
(ii) Clinical manifestations.
Most patients with thyroid nodules have no clinical symptoms. They are usually detected on physical examination by palpation of the thyroid and ultrasound of the neck. Most thyroid nodules are benign, with malignant tumors accounting for about
= “wp-image-30268″ src=”https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225872-word-image-1.png” /> . In combination with hyper- or hypothyroidism, the corresponding clinical manifestations may occur. Benign nodules or malignant tumors of the thyroid gland can increase in size and may cause compression, often against the
It may compress the trachea and esophagus and displace the trachea and esophagus. If the malignant tumor locally encroaches on the surrounding organs, symptoms such as hoarseness, dysphagia, hemoptysis and dyspnea may also occur. MTC tumor cells secrete active substances such as calcitonin and 5-hydroxytryptamine, which can cause diarrhea, palpitations, and flushing.
The signs of thyroid cancer are mainly enlargement or nodule of thyroid gland with irregular shape, fixed adhesion to surrounding tissues, and gradually increasing in size, hard texture and unclear boundary, initially moving up and down with swallowing movement.
The nodules may initially move up and down with swallowing movements, but later they are mostly immobile. If the node is associated with cervical lymph node metastasis, the lymph nodes in the neck may be enlarged by palpation. Compression or invasion of sympathetic nerves may cause Horner syndrome.
- Invasion and metastasis
- Local invasion: Thyroid cancer can locally invade the recurrent laryngeal nerve, trachea, esophagus, cricoid cartilage, and larynx, even to the prevertebral tissues, and laterally to the internal jugular vein, vagus nerve, or common carotid artery in the cervical sheath.
- Regional lymph node metastasis: PTC is prone to early regional lymphatic metastasis, and most patients with PTC already have cervical lymphatic metastasis at the time of diagnosis. lymph node metastasis is usually ipsilateral to the primary focus and follows a lymphatic drainage pathway from station to station, with lymphatic drainage generally first to the paratracheal lymph nodes and then to the internal jugular vein lymph node chain (regions II-IV) and posterior jugular lymph nodes
.
(The most common site of metastasis is region VI, followed by regions III, IV, II, and V. When lymph node metastasis in the lateral cervical region occurs in PTC, it is predominantly multi-regional metastasis, and only single-region metastasis is less common. Lymphatic metastases in region I are rare (<3  ). Rare lymph node metastasis sites include retropharyngeal/parapharyngeal, intraparotid, and axillary.
). Rare lymph node metastasis sites include retropharyngeal/parapharyngeal, intraparotid, and axillary.
- Distant metastases: The lung is a common distant metastatic organ for thyroid cancer. Metastases to bone, liver, and intracranial sites can also occur in thyroid cancer. Follicular thyroid cancer, poorly differentiated thyroid cancer, and undifferentiated cancer have a higher risk of distant metastasis.
- Common complications
Most thyroid cancers are differentiated thyroid cancers that grow relatively slowly, and serious complications are rare. It may cause hoarseness, dyspnea, hemoptysis, etc. due to invasion of the laryngeal nerve, trachea and other surrounding organs.
ATC is rapidly progressing and may cause severe respiratory distress.
Routine laboratory tests
The purpose is to understand the patient’s general condition and the need for appropriate therapeutic measures, including blood work, liver and kidney function, and thyroid function. If invasive testing or surgical treatment is required, coagulation and viral markers are also required. For patients with DTC who require thyroid stimulating hormone (TSH) suppression below the lower limit of the normal reference range (especially in postmenopausal women), pre-treatment baseline bone mineralization status should be evaluated and monitored regularly, depending on medical conditions; serum calcium/phosphorus, 24-hour urine calcium/phosphorus, and bone turnover biochemistry may be used.
serum calcium/phosphorus, 24-hour urinary calcium/phosphorus, and biochemical markers of bone turnover.
- Thyroid hormone, thyroid autoantibody, and tumor marker testing
- Thyroid hormone testing: This includes measurement of thyroxine (T4), triiodothyronine (T3), free T4 (FT4) and free triiodothyronine (FT3) in the blood, and TSH. TSH testing is an important initial screening test to clarify thyroid function. In patients with thyroid cancer treated with TSH suppression, blood thyroid hormone levels also need to be tested regularly and levothyroxine (L-T4) adjusted according to the test results.
- Thyroid autoantibody testing: The main autoantibodies associated with autoimmune thyroid disease are anti-thyroglobulin antibodies (TgAb), thyroid peroxisome antibodies (thyroid
- Differentiation of benign and malignant nodules: Ultrasonography is simple and noninvasive, with high specificity and sensitivity for thyroid nodules, and can clearly show the boundary, morphology, size and internal structure of nodules.Ultrasound of the neck. Ultrasound of the neck should determine the size, number, location, cystic solidity, shape, borders, calcification, blood supply, and relationship to surrounding tissues, as well as the presence of abnormal lymph nodes in the neck and their location, size, morphology, blood flow, and structural features.
Other malignant signs include solid hypoechoic nodules, halo defects, extrathyroidal invasion, and abnormal ultrasound signs in the cervical lymph nodes. Other signs of cervical lymph node abnormalities include microcalcifications, cystic changes, hyperechogenicity, and peripheral blood flow in the lymph nodes, as well as rounded lymph nodes, irregular or blurred borders, uneven internal echogenicity, loss of lymphatic portals, or poorly delineated corticomedullary structures.
The ability to identify thyroid nodules and lymph nodes correlates with the clinical experience of the sonographer. Thyroid imaging reporting and data system (TI-RADS)
data system (TI-RADS), which assesses the malignancy of thyroid nodules, helps standardize thyroid ultrasound reporting and is recommended for use when available. However, the TI- RADS classification is not unified at present, and the criteria can be referred to Table 1. Ultrasonography and ultrasound elastography can be used as complementary tools, but are not recommended for routine application.
Table 1 TI-RADS classification for ultrasound evaluation of thyroid nodules
Classification Evaluation Ultrasound presentation Risk of malignancy-
- No nodules Diffuse lesions 0
- Negative Normal thyroid (or postoperative) 0
- Benign Cystic or solid predominantly benign nodules with regular morphology and well-defined borders
0
-
- Probably benign
Atypical benign nodule <5

-
- Suspicious malignancy
Signs of malignancy: substantial, hypoechoic or extremely

 hypoechoic, microcalcifications, faint border/micro 5 to
hypoechoic, microcalcifications, faint border/micro 5 to
lobulated, aspect ratio >1 85 4a with 1 malignant sign 5 to
4a with 1 malignant sign 5 to
10
4b With 2 signs of malignancy 10 to
50
 4c with 3 to 4 signs of malignancy signs 50 to
4c with 3 to 4 signs of malignancy signs 50 to
85
5 Malignant More than 4 signs of malignancy, especially with micro 85  ~
~>
Calcareous and differential lobers 100 
>
6 Malignant Pathologically confirmed malignant lesions None - Ultrasound-guided fine-needle aspiration biopsy: Fine-needle aspiration biopsy (FNAB) uses a fine needle to puncture thyroid nodules to obtain cellular components and diagnose the nature of the lesion by cytology. Ultrasound guidance can improve the success rate and diagnostic accuracy of extraction, as well as the protection of important tissue structures during puncture and the determination of hematoma after puncture, and is recommended as a further diagnostic method to determine the benignity and malignancy of thyroid nodules.
The FNAB can be divided into negative pressure and nonnegative pressure FNAs, which can be selected or combined as appropriate in clinical practice. To improve the accuracy of FNAB, the following methods can be used: repeated puncture of multiple sites in the same nodule; sampling in parts of the nodule that are suspicious on ultrasound; and sampling in the solid part of a cystic nodule, along with cytology of the cyst fluid.
The indications for ultrasound-guided FNAB (US-FNAB) of thyroid nodules: US-FNAB is recommended for thyroid nodules >1 cm in diameter with ultrasound assessment of malignancy; for thyroid nodules ≤1 cm in diameter, puncture biopsy is not routinely recommended, but US-FNAB may be considered if one of the following conditions exists FNAB: ultrasound suggestive of a malignant thyroid nodule; abnormal cervical lymph nodes on ultrasound; history of radiation exposure to the neck or radiation contamination in childhood; family history of thyroid cancer or thyroid cancer syndrome; positive 18F-fluorodeoxyglucose (18F-FDG); abnormal serum calcitonin level elevated.
(ii) Exclusion indications for US-FNAB: thyroid nodules with autonomic uptake confirmed by thyroid nuclide imaging; nodules with purely cystic nature suggested by ultrasonography.
(iii) Contraindications to US-FNAB for thyroid nodules: bleeding tendency, significantly prolonged bleeding and clotting times, significantly reduced prothrombin activity; possible damage to adjacent vital organs through the puncture needle route; long-term use of anticoagulants; difficulty with frequent coughing and swallowing; refusal of invasive testing; infection at the puncture site that must be treated before puncture can be performed. Women who are menstruating are relatively contraindicated.- Ultrasound during follow-up: In patients who have not undergone surgical treatment, ultrasound follow-up should be performed to detect any increase in the size of the original nodule or any of the aforementioned signs of malignancy. Increase in nodule size
-
- Acquisition of FNA: There are two methods of acquiring thyroid FNA, palpation-guided FNA and ultrasound-guided FNA. Palpation-guided FNA is only indicated for palpable solid nodules; ultrasound-guided FNA should be performed for nonpalpable nodules, cystic nodules, or nodules with previous unsatisfactory FNA.
- Thyroid FNA is commonly performed with a needle with an outer diameter of 22 to 27 G,
- Production of FNA: Production techniques for cellular specimens include conventional smear, liquid-based production, and cell block sectioning. Conventional smears are the most common method of preparation, in which cells obtained from FNA are applied directly to a slide, dried, and fixed in alcohol. If the explanted material is cystic fluid, liquid-based filming will enrich the cells in the cystic fluid, resulting in a more abundant smear than conventional smears. For rare types of thyroid tumors, such as medullary carcinoma, undifferentiated carcinoma, and metastatic carcinoma, it is best to add a cell block for immunocytochemical testing. The combination of conventional smears and liquid-based films can improve diagnostic accuracy, and on-site evaluation of cellular specimens can be performed in units where available to improve the satisfactory rate of sampling.
- Cytopathology Diagnostic Reporting: The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is used for cytopathology diagnostic reporting, in which cytologic diagnoses are classified into 6 levels: Level I, non-diagnostic/unsatisfactory; Level II, benign. unsatisfactory; grade II, benign; grade III, atypical cells of unknown significance/follicular lesions of unknown significance; grade IV, follicular neoplasm/suspicious follicular neoplasm; grade V, suspicious malignancy; and grade VI, malignant (Table 2). Patients with different cytologic diagnostic grades have different risks of malignancy and different clinical management measures
- Importance of standardized pathologic diagnosis: The biological behavior of different pathologic types of thyroid tumors varies widely, from benign thyroid adenomas and junctional thyroid tumors to thyroid cancer, which can have important implications for patient prognosis and treatment. Lymph node metastasis in thyroid cancer is also important for patient management strategies. In order to better assist clinicians in developing precise treatment plans, it is important that different levels of hospitals, different
- Preoperative aspiration pathology: Preoperative B-ultrasound localized coarse needle aspiration allows collection of tumor tissue for histopathologic diagnosis, which can be definitive when the specimen is adequate and the morphology is typical. Because of the obvious advantages of FNA in the diagnosis of thyroid cancer, histologic aspiration is generally not used as a routine test, but can be used as a complementary application in some cases of suspicious rare types.
- Intraoperative frozen pathology: The purpose is to characterize thyroid nodules that have not been diagnosed preoperatively by puncture or have an unclear pathology, and to clarify the presence or absence of lymph node metastases to determine the type of thyroidectomy or the extent of lymph node dissection.
- Postoperative paraffin pathology diagnosis:
- Cautions for sampling: ① Make parallel sections at 2-3 mm intervals perpendicular to the long axis of the specimen;
- Take a parallel section every 2 to 3 mm in the long axis of the specimen perpendicular to the long axis of the specimen.
- Diagnostic guidelines: i.e., what should be included in the pathology report: (1) location of the tumor, number and size of lesions; (2) pathological type, subtype, fibrosis and calcification; (3) choroidal and nerve invasion (small nerve invasion near the perineurium or branches of the laryngeal recurrent nerve); (4) involvement of the thyroid perineurium; (5) invasion of the strap muscles; (6) presence of other lesions in the surrounding thyroid gland such as chronic lymphocytic thyroiditis, nodular goiter
- Thyroid adenoma: This disease is most often seen in young people aged 20 to 30 years, mostly as a single nodule with clear borders, smooth surface, slow growth, sudden enlargement often with intracapsular hemorrhage, and no cervical lymph node metastasis or distant metastasis.
- Nodular goiter: Most often seen in women over middle age, the disease can last for decades. Multiple nodules in both lobes of the gland are common, varying in size, and may be cystic. A large mass may compress the trachea and displace the trachea, and the patient may have difficulty breathing. The probability of carcinoma is low, but it is seen in older patients with larger masses and a longer course of disease, which is manifested by a significant acceleration in the rate of mass enlargement.
- Subacute thyroiditis: This may be caused by a viral infection and may last for several weeks or months. It is often preceded by a history of respiratory infection, may be associated with mild fever, localized pain that is apparent when swallowing and may radiate to the ear, diffuse enlargement of the thyroid gland, or asymmetric nodular masses with pressure pain. It is a self-limiting disease that resolves spontaneously over a period of several weeks. A small number of patients require surgery to rule out thyroid cancer.
- Chronic lymphocytic thyroiditis (Hashimoto’s thyroiditis): Chronic progressive bilateral enlargement of the thyroid gland, sometimes indistinguishable from thyroid cancer, usually without conscious symptoms and with elevated autoantibody titers. The disease is mostly treated conservatively and is more sensitive to adrenocorticosteroids, sometimes requiring surgery or a small amount of x-ray radiotherapy.
- Fibrotic thyroiditis: The thyroid gland is generally enlarged and hard as wood, but often retains its original shape. It is often fixed to surrounding tissue and produces symptoms of compression, and is often difficult to distinguish from cancer. Surgical exploration and removal of the isthmus is possible when symptoms of tracheal compression are present.
- Columnar cell subtype: This rare subtype consists of pseudostratified columnar cells that often lack the typical PTC nuclear features and occasionally show subnuclear vacuoles and clear cytoplasm, similar to endometrial or intestinal adenocarcinoma. In some cases, immunohistochemical staining is positive for CDX2 and TTF1 is positive to varying degrees. The prognosis may be related to tumor size and extraglandular spread, but not to the type itself.
- Sieve-mulberry-like subtype: This subtype is considered a distinct subtype of thyroid cancer that occurs almost exclusively in women, is usually associated with familial adenomatous polyposis, has germline mutations in the APC gene, and can also occur in sporadic cases. Sporadic cases are usually solitary and have an excellent prognosis, requiring only lobectomy. Familial cases often have multiple foci and are often associated with colonic polyposis and require APC genetic testing. Tumors are usually encapsulated lesions with a mixture of sieve, follicular, papillary, beam-like, solid, and mulberry-like structures. Envelope/vascular invasion is common. The lumina of sieve-like structures are large and unrounded and lack intraluminal glia. The nucleus is not particularly clear. Immunostaining is often mottled positive for TTF1. TG is focal or weakly positive. β-linked protein shows characteristic nuclear positivity. Mulberry-like structures express a broad spectrum of CK,
- Shoe peg type: a rare subtype of PTC with aggressive behavior and relatively poor prognosis. Diagnosis requires that at least 30% of the tumor cells exhibit bootstrap micropapillary features. The presence of a small number of bootstrap micropapillary structures is also significant and should be noted in the pathology report. Compared to classic PTC, bootstrap PTC often shows extra-glandular spread, lymph node metastases or distant metastases, and responds poorly to radioiodine therapy, resulting in increased mortality. Molecular detection of BARF mutations is predominant.
- FTC and its subtypes
- AJCC staging
- Lymph node metastasis: The prognostic role of regional lymphatic metastasis is controversial. There is evidence to support that regional lymph node metastases do not affect recurrence or survival. There is also evidence to support that lymph node metastases are a high risk factor for local recurrence and cancer-related mortality. There is a correlation between lymphatic metastases and distant metastases, especially those with bilateral cervical lymph node metastases, or extraperitoneal invasion of lymph nodes, or mediastinal lymph node metastases.
- Distant metastases: In DTC, distant metastases are a major cause of death. Approximately 10
 of PTC, 25 < img class="wp-image-30373" src="https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225930-word-image.png" /> of FTC will develop distant metastases. Distant metastases in eosinophilic glands
of PTC, 25 < img class="wp-image-30373" src="https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225930-word-image.png" /> of FTC will develop distant metastases. Distant metastases in eosinophilic glands - Surgical treatment of differentiated thyroid cancer
- Management of the primary focus: lesions with a T grade of T1 or T2, which are mostly confined to one lobe, are recommended for resection of the affected lobe and isthmus. For some patients with high-risk factors, total thyroidectomy is also indicated. These risk factors include multifocal cancer, lymph node metastases, distant metastases, family history, and early childhood exposure to ionizing radiation. Total thyroidectomy is also indicated in some cases where postoperative nuclear therapy is considered necessary. For tumors located in the isthmus, extended isthmus resection is indicated for smaller tumors, while total thyroidectomy may be considered for larger tumors or those with lymph node metastases.
- Medium-risk stratification
- The 2015 ATA Guidelines strongly recommend 131I therapy for patients stratified for high risk of recurrence
- 131I therapy may be considered for patients in intermediate-risk stratification with microscopic thyroid exenteration
- 131I therapy is not recommended in low-risk groups with ≤5 lymph node involvement (no extra-pericyclic invasion, lesions <0.2 cm). To facilitate follow-up by monitoring serum Tg levels and 131I whole-body imaging, 131I thyroid clearance therapy is feasible.
- Women during pregnancy or lactation.
- People who are planning a pregnancy within 6 months.
- Recommended 30mCi for thyroid clearance therapy in intermediate- and low-risk patients.
- For intermediate- and high-risk patients with suspected or proven microscopic residual disease or highly aggressive histologic subtypes (hypercellular, columnar cell, etc.) without distant metastases, an adjuvant 131I dose of 150 mCi is recommended.
- A higher dose of 131I is considered for patients with more residual thyroid tissue or focal clearance after incomplete/near-total thyroidectomy
- Thyroid clearance should be combined with focal clearance therapy at a 131I dose of 100-200 mCi in patients with residual surgically unresected DTC tissue in the neck, with inoperable or patient-refused cervical lymph nodes or distant metastases, and with unexplained elevated serum Tg levels after total thyroidectomy, especially irritant Tg. For adolescents, women of childbearing age, elderly patients, and. The dose of 131I may be reduced as appropriate in patients with mild to moderate renal impairment.
- For high-risk patients, an initial TSH target value of <0.1 mU/L is recommended.
- For intermediate-risk patients, an initial TSH target of 0.1 to 0.5 mU/L is recommended.
- For low-risk patients with undetectable serum Tg, a TSH target of 0.5 to 2 mU/L is recommended, regardless of whether 131I thyroid clearance therapy has been administered.
- For low-risk patients with undetectable serum Tg, a TSH target of 0.5 to 2 mU/L is recommended.
- For low-risk patients who have had 131I thyroid clearance and have low Tg levels or for low-risk patients who have not had 131I thyroid clearance and have slightly higher Tg levels, a TSH target of 0.1 to 0.5 mU/L is recommended;
- For low-risk patients who have had 131I thyroid clearance and have low Tg levels, a TSH target of 0.1 to 0.5 mU/L is recommended.
- For patients with lobectomy, a TSH target of 0.5 to 2 mU/L is recommended.
- For patients with an unsatisfactory outcome on imaging assessment, a TSH target of <0.1 mU/L is recommended in the absence of specific contraindications.
- For patients with an unsatisfactory outcome on imaging assessment, a TSH target of <0.1 mU/L is recommended in the absence of specific contraindications.
- For patients with unsatisfactory efficacy on serologic assessment, a TSH target of 0.1 to 0.5 mU/L is recommended based on initial ATA risk stratification, Tg levels, trends in Tg changes, and adverse effects of TSH suppressive therapy.
- For patients initially rated as high risk but with a satisfactory treatment response (clinical or serologic disease-free status) or unclear efficacy, a TSH target of 0.1 to 0.5 mU/L for up to 5 years with subsequent reduction in TSH suppression is recommended.
- For patients with a satisfactory treatment response (clinical or serologic disease-free status) or unclear efficacy, particularly those at low risk of relapse, a TSH target of 0.5 to 2 mU/L is recommended.
- For patients without 131I thyroid clearance or adjuvant therapy and with satisfactory or unclear outcome, meeting a negative neck ultrasound, low or undetectable suppressive Tg, and no trend toward increased Tg or TgAb, a TSH target of 0.5 to 2 mU/L is recommended.
- For the treatment of pulmonary metastases where the lesion is still iodine uptake and appears clinically effective, every
- For bone metastases, the dose is 100 to 200 mCi.
- Surgery or stereotactic external radiotherapy is recommended as the first consideration for central nervous system metastases.
- Continue TSH suppression therapy with close follow-up for patients with sTg <10 ng/ml from discontinuation of L-T4 or sTg <5 ng/ml from application of rhTSH, but empiric 131I therapy is feasible if there is a progressive increase in serum Tg or other evidence of disease progression (PD).
- For patients with sTg >10ng/ml from discontinuation of L-T4 or sTg >5ng/ml from rhTSH application, with persistently elevated Tg or TgAb levels and negative neck and chest imaging, 18F-FDG PET-CT, empiric 131I treatment at 100-200mCi is feasible, but if Rx-WBS is still negative However, if Rx-WBS remains negative, the patient is classified as iodine-refractory DTC and 131I therapy needs to be discontinued.
- Figure 3. Indications for radiotherapy for MTC
- Intensity-modulated radiation therapy (IMRT) and 3D conformal radiotherapy:
- Simulated CT localization:
- Target area development (Figure 4): there is considerable controversy regarding target area determination. Some studies suggest that small-field treatment can be used, with adequate attention to surgeons for external radiation to areas of high postoperative incidence and areas that are not easily resected surgically. Some investigators believe that large-field radiation should be used, with the option of treating areas of cervical lymph node drainage.
- High-risk area (CTV1): includes the thyroid area, surrounding lymph node drainage areas, and all areas with pathologically confirmed positive lymph nodes.
- Selective treatment area (CTV2): includes areas of lymph node drainage II-VI and upper mediastinal lymph nodes without pathologic confirmation but with potential metastasis, with a lower rate of metastasis in the retropharyngeal lymph nodes and in area I. However, the probability of metastasis in the retropharyngeal lymph nodes increases significantly if there are lymph nodes in area II, and the probability of metastasis in area Ib is increased if there are large lymph nodes in area IIa
- Localization: The same body position as for IMRT is recommended, using a simulated CT for localization and outlining the field on the planning system. Without analog CT equipment, X-ray orthogonal images can be used for field sketching.
- Radiographic field design:
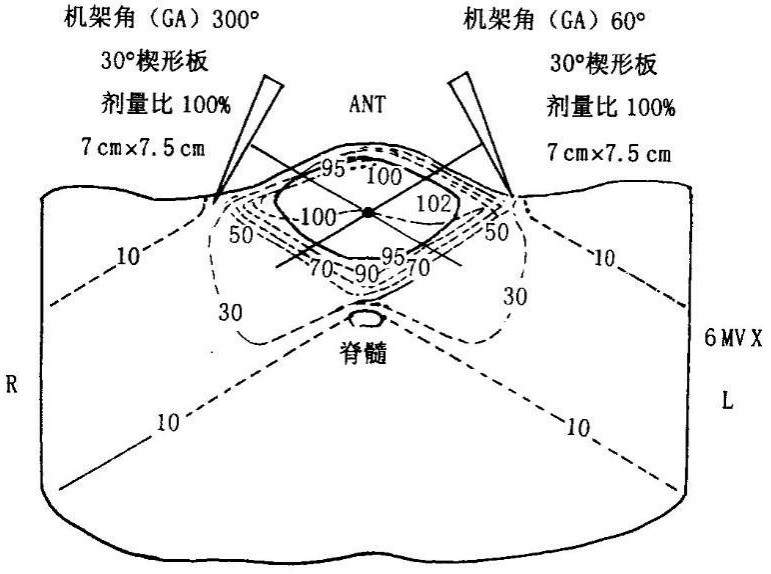 Two anterior oblique field cross-angle wedge Illumination technique: see Figure 6.
Two anterior oblique field cross-angle wedge Illumination technique: see Figure 6.- Irradiation dose: according to the radiotherapy protocol (macro-segmentation protocol and conventional segmentation radiotherapy prescription
- Acute complications: 1 to 2 degree reactions are more common in about 80
 or more, including pharyngitis, mucositis, dry mouth, taste changes, dysphagia, painful swallowing, radiolucent skin
or more, including pharyngitis, mucositis, dry mouth, taste changes, dysphagia, painful swallowing, radiolucent skin - Zheng Qi deficiency
- Liver and kidney deficiency
- Liver depression and qi stagnation
- For patients with distant metastatic high-risk differentiated thyroid cancer, surgery + postoperative 131I therapy + postoperative TSH suppression is the primary combination treatment modality.
- For localized lesions that are not surgically resectable, local radiofrequency ablation or external radiotherapy may be considered.
- The treatment of MTC should be primarily surgical, without TSH suppression, but with thyroxine replacement therapy.
- For ATC, external radiotherapy + surgery is preferred in the absence of distant metastases and airway obstruction
- For patients with DTC who have had total thyroid clearance (after surgery + 131I thyroid clearance), serum Tg levels should be measured regularly (along with TgAb), and the same test reagents are recommended. Long-term follow-up of serum Tg begins 6 months after 131I thyroid clearance therapy, when basal Tg or sTg is measured. sTg is repeated 12 months after 131I therapy, and basal Tg is repeated every 6 to 12 months thereafter. sTg may be repeated 3 years after thyroid clearance therapy for those at intermediate or high risk of recurrence.
- Neck ultrasound should be performed periodically during DTC follow-up to assess the status of the thyroid bed and lymph nodes in the central and lateral cervical regions of the neck. The first postoperative ultrasound examination is recommended 3 months after surgery in high-risk patients and 6 months after surgery in intermediate- and low-risk patients. If suspicious lesions are found, the examination interval can be shortened as appropriate. Ultrasound-guided puncture biopsy and/or Tg testing of the puncture eluate is indicated for suspicious lymph nodes.
- Patients with DTC may be followed up with Dx-WBS optionally after surgery and 131I thyroid clearance, depending on the risk of recurrence.
- 18F-FDG PET is not currently recommended for routine use in DTC follow-up, but may be considered in the following situations: (1) to assist in finding and localizing the lesion when serum Tg levels are elevated (>10 ng/ml) and Dx-WBS is negative; (2) to evaluate and monitor the disease in those with lesions that do not uptake iodine; and (3) to evaluate and monitor the disease in invasive or metastatic DTC.
- Long-term follow-up of DTC should also include the following: (1) long-term safety of 131I therapy: including effects on secondary tumors, reproductive system. However, over-screening and screening should be avoided; (ii) the effect of TSH suppression therapy: including whether TSH suppression therapy is achieved and the side effects of therapy; (iii) concomitant diseases in DTC patients: because some concomitant diseases (e.g., cardiac disease, other malignancies, etc.) may be of higher clinical urgency than DTC itself, the condition of these concomitant diseases should also be dynamically observed during long-term follow-up.
- Local invasion: Thyroid cancer can locally invade the recurrent laryngeal nerve, trachea, esophagus, cricoid cartilage, and larynx, even to the prevertebral tissues, and laterally to the internal jugular vein, vagus nerve, or common carotid artery in the cervical sheath.
- Regional lymph node metastasis: PTC is prone to early regional lymphatic metastasis, and most patients with PTC already have cervical lymphatic metastasis at the time of diagnosis. lymph node metastasis is usually ipsilateral to the primary focus and follows a lymphatic drainage pathway from station to station, with lymphatic drainage generally first to the paratracheal lymph nodes and then to the internal jugular vein lymph node chain (regions II-IV) and posterior jugular lymph nodes
- Distant metastases: The lung is a common distant metastatic organ for thyroid cancer. Metastases to bone, liver, and intracranial sites can also occur in thyroid cancer. Follicular thyroid cancer, poorly differentiated thyroid cancer, and undifferentiated cancer have a higher risk of distant metastasis.
- Common complications
- Thyroid hormone testing: This includes measurement of thyroxine (T4), triiodothyronine (T3), free T4 (FT4) and free triiodothyronine (FT3) in the blood, and TSH. TSH testing is an important initial screening test to clarify thyroid function. In patients with thyroid cancer treated with TSH suppression, blood thyroid hormone levels also need to be tested regularly and levothyroxine (L-T4) adjusted according to the test results.
- Thyroid autoantibody testing: The main autoantibodies associated with autoimmune thyroid disease are anti-thyroglobulin antibodies (TgAb), thyroid peroxisome antibodies (thyroid
- Differentiation of benign and malignant nodules: Ultrasonography is simple and noninvasive, with high specificity and sensitivity for thyroid nodules, and can clearly show the boundary, morphology, size and internal structure of nodules.Ultrasound of the neck. Ultrasound of the neck should determine the size, number, location, cystic solidity, shape, borders, calcification, blood supply, and relationship to surrounding tissues, as well as the presence of abnormal lymph nodes in the neck and their location, size, morphology, blood flow, and structural features.
Other malignant signs include solid hypoechoic nodules, halo defects, extrathyroidal invasion, and abnormal ultrasound signs in the cervical lymph nodes. Other signs of cervical lymph node abnormalities include microcalcifications, cystic changes, hyperechogenicity, and peripheral blood flow in the lymph nodes, as well as rounded lymph nodes, irregular or blurred borders, uneven internal echogenicity, loss of lymphatic portals, or poorly delineated corticomedullary structures.
The ability to identify thyroid nodules and lymph nodes correlates with the clinical experience of the sonographer. Thyroid imaging reporting and data system (TI-RADS)
data system (TI-RADS), which assesses the malignancy of thyroid nodules, helps standardize thyroid ultrasound reporting and is recommended for use when available. However, the TI- RADS classification is not unified at present, and the criteria can be referred to Table 1. Ultrasonography and ultrasound elastography can be used as complementary tools, but are not recommended for routine application.
Table 1 TI-RADS classification for ultrasound evaluation of thyroid nodules
Classification Evaluation Ultrasound presentation Risk of malignancy-
- No nodules Diffuse lesions 0
- Negative Normal thyroid (or postoperative) 0
- Benign Cystic or solid predominantly benign nodules with regular morphology and well-defined borders
0
-
- Probably benign
Atypical benign nodule <5

-
- Suspicious malignancy
Signs of malignancy: substantial, hypoechoic or extremely

 hypoechoic, microcalcifications, faint borders/micro 5 to
hypoechoic, microcalcifications, faint borders/micro 5 to
lobulated, aspect ratio >1 85 4a with 1 malignant sign 5 to
4a with 1 malignant sign 5 to
10
4b With 2 signs of malignancy 10 to
50
 4c with 3 to 4 signs of malignancy 50 to
4c with 3 to 4 signs of malignancy 50 to
85
5 Malignant More than 4 signs of malignancy, especially with micro 85  ~
~Calcifiers and Differential Leafers 100 
6 Malignant Pathologically confirmed malignant lesions None - Ultrasound-guided fine-needle aspiration biopsy: Fine-needle aspiration biopsy (FNAB) uses a fine needle to puncture thyroid nodules to obtain cellular components and diagnose the nature of the lesion by cytology. Ultrasound guidance can improve the success rate and diagnostic accuracy of extraction, as well as the protection of important tissue structures during puncture and the determination of hematoma after puncture, and is recommended as a further diagnostic method to determine the benignity and malignancy of thyroid nodules.
The FNAB can be divided into negative pressure and nonnegative pressure FNAs, which can be selected or combined as appropriate in clinical practice. To improve the accuracy of FNAB, the following methods can be used: repeated puncture of multiple sites in the same nodule; sampling in parts of the nodule that are suspicious on ultrasound; and sampling in the solid part of a cystic nodule, along with cytology of the cyst fluid.
The indications for ultrasound-guided FNAB (US-FNAB) of thyroid nodules: US-FNAB is recommended for thyroid nodules >1 cm in diameter with ultrasound assessment of malignancy; for thyroid nodules ≤1 cm in diameter, puncture biopsy is not routinely recommended, but US-FNAB may be considered if one of the following conditions exists FNAB: ultrasound suggestive of a malignant thyroid nodule; abnormal cervical lymph nodes on ultrasound; history of radiation exposure to the neck or radiation contamination in childhood; family history of thyroid cancer or thyroid cancer syndrome; positive 18F-fluorodeoxyglucose (18F-FDG); abnormal serum calcitonin level elevated.
(ii) Exclusion indications for US-FNAB: thyroid nodules with autonomic uptake confirmed by thyroid nuclide imaging; nodules with purely cystic nature suggested by ultrasonography.
(iii) Contraindications to US-FNAB for thyroid nodules: bleeding tendency, significantly prolonged bleeding and clotting times, significantly reduced prothrombin activity; possible damage to adjacent vital organs through the puncture needle route; long-term use of anticoagulants; difficulty with frequent coughing and swallowing; refusal of invasive testing; infection at the puncture site that must be treated before puncture can be performed. Women who are menstruating are relatively contraindicated.- Ultrasound during follow-up: In patients who have not undergone surgical treatment, ultrasound follow-up should be performed to detect any increase in the size of the original nodule or any of the aforementioned signs of malignancy. Increase in nodule size
-
- Acquisition of FNA: There are two methods of acquiring thyroid FNA, palpation-guided FNA and ultrasound-guided FNA. Palpation-guided FNA is only indicated for palpable solid nodules; ultrasound-guided FNA should be performed for nonpalpable nodules, cystic nodules, or nodules with previous unsatisfactory FNA.
- Thyroid FNA is commonly performed with a needle with an outer diameter of 22 to 27 G,
- Production of FNA: Production techniques for cellular specimens include conventional smear, liquid-based production, and cell block sectioning. Conventional smears are the most common method of preparation, in which cells obtained from FNA are applied directly to a slide, dried, and fixed in alcohol. If the explanted material is cystic fluid, liquid-based filming will enrich the cells in the cystic fluid, resulting in a more abundant smear than conventional smears. For rare types of thyroid tumors, such as medullary carcinoma, undifferentiated carcinoma, and metastatic carcinoma, it is best to add a cell block for immunocytochemical testing. The combination of conventional smears and liquid-based films can improve diagnostic accuracy, and on-site evaluation of cellular specimens can be performed in units where available to improve the satisfactory rate of sampling.
- Cytopathology Diagnostic Reporting: The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is used for cytopathology diagnostic reporting, in which cytologic diagnoses are classified into 6 levels: Level I, non-diagnostic/unsatisfactory; Level II, benign. unsatisfactory; grade II, benign; grade III, atypical cells of unknown significance/follicular lesions of unknown significance; grade IV, follicular neoplasm/suspicious follicular neoplasm; grade V, suspicious malignancy; and grade VI, malignant (Table 2). Patients with different cytologic diagnostic grades have different risks of malignancy and different clinical management measures
- Importance of standardized pathologic diagnosis: The biological behavior of different pathologic types of thyroid tumors varies widely, from benign thyroid adenomas and junctional thyroid tumors to thyroid cancer, which can have important implications for patient prognosis and treatment. Lymph node metastasis in thyroid cancer is also important for patient management strategies. In order to better assist clinicians in developing precise treatment plans, it is important that different levels of hospitals, different
- Preoperative aspiration pathology: Preoperative B-ultrasound localized coarse needle aspiration allows collection of tumor tissue for histopathologic diagnosis, which can be definitive when the specimen is adequate and the morphology is typical. Because of the obvious advantages of FNA in the diagnosis of thyroid cancer, histologic aspiration is generally not used as a routine test, but can be used as a complementary application in some cases of suspicious rare types.
- Intraoperative frozen pathology: The purpose is to characterize thyroid nodules that have not been diagnosed preoperatively by puncture or have an unclear pathology, and to clarify the presence or absence of lymph node metastases to determine the type of thyroidectomy or the extent of lymph node dissection.
- Postoperative paraffin pathology diagnosis:
- Cautions for sampling: ① Make parallel sections at 2-3 mm intervals perpendicular to the long axis of the specimen;
- Take a parallel section every 2 to 3 mm in the long axis of the specimen perpendicular to the long axis of the specimen.
- Diagnostic guidelines: i.e., what should be included in the pathology report: (1) location of the tumor, number and size of lesions; (2) pathological type, subtype, fibrosis and calcification; (3) choroidal and nerve invasion (small nerve invasion near the perineurium or branches of the laryngeal recurrent nerve); (4) involvement of the thyroid perineurium; (5) invasion of the strap muscles; (6) presence of other lesions in the surrounding thyroid gland such as chronic lymphocytic thyroiditis, nodular goiter
- Thyroid adenoma: This disease is most often seen in young people aged 20 to 30 years, mostly as a single nodule with clear borders, smooth surface, slow growth, sudden enlargement often with intracapsular hemorrhage, and no cervical lymph node metastasis or distant metastasis.
- Nodular goiter: Most often seen in women over middle age, the disease can last for decades. Multiple nodules in both lobes of the gland are common, varying in size, and may be cystic. A large mass may compress the trachea and displace the trachea, and the patient may have difficulty breathing. The probability of carcinoma is low, but it is seen in older patients with larger masses and a longer course of disease, which is manifested by a significant acceleration in the rate of mass enlargement.
- Subacute thyroiditis: This may be caused by a viral infection and may last for several weeks or months. It is often preceded by a history of respiratory infection, may be associated with mild fever, localized pain that is apparent when swallowing and may radiate to the ear, diffuse enlargement of the thyroid gland, or asymmetric nodular masses with pressure pain. It is a self-limiting disease that resolves spontaneously over a period of several weeks. A small number of patients require surgery to rule out thyroid cancer.
- Chronic lymphocytic thyroiditis (Hashimoto’s thyroiditis): Chronic progressive bilateral enlargement of the thyroid gland, sometimes indistinguishable from thyroid cancer, usually without conscious symptoms and with elevated autoantibody titers. The disease is mostly treated conservatively and is more sensitive to adrenocorticosteroids, sometimes requiring surgery or a small amount of x-ray radiotherapy.
- Fibrotic thyroiditis: The thyroid gland is generally enlarged and hard as wood, but often retains its original shape. It is often fixed to surrounding tissue and produces symptoms of compression, and is often difficult to distinguish from cancer. Surgical exploration and removal of the isthmus is possible when symptoms of tracheal compression are present.
- Columnar cell subtype: This rare subtype consists of pseudostratified columnar cells that often lack the typical PTC nuclear features and occasionally show subnuclear vacuoles and clear cytoplasm, similar to endometrial or intestinal adenocarcinoma. In some cases, immunohistochemical staining is positive for CDX2 and TTF1 is positive to varying degrees. The prognosis may be related to tumor size and extraglandular spread, but not to the type itself.
- Sieve-mulberry-like subtype: This subtype is considered a distinct subtype of thyroid cancer that occurs almost exclusively in women, is usually associated with familial adenomatous polyposis, has germline mutations in the APC gene, and can also occur in sporadic cases. Sporadic cases are usually solitary and have an excellent prognosis, requiring only lobectomy. Familial cases often have multiple foci and are often associated with colonic polyposis and require APC genetic testing. Tumors are usually encapsulated lesions with a mixture of sieve, follicular, papillary, beam-like, solid, and mulberry-like structures. Envelope/vascular invasion is common. The lumina of sieve-like structures are large and unrounded and lack intraluminal glia. The nucleus is not particularly clear. Immunostaining is often mottled positive for TTF1. TG is focal or weakly positive. β-linked protein shows characteristic nuclear positivity. Mulberry-like structures express a broad spectrum of CK,
- Shoe peg type: a rare subtype of PTC with aggressive behavior and relatively poor prognosis. Diagnosis requires that at least 30% of the tumor cells exhibit bootstrap micropapillary features. The presence of a small number of bootstrap micropapillary structures is also significant and should be noted in the pathology report. Compared to classic PTC, bootstrap PTC often shows extra-glandular spread, lymph node metastases or distant metastases, and responds poorly to radioiodine therapy, resulting in increased mortality. Molecular detection of BARF mutations is predominant.
- FTC and its subtypes
- AJCC staging
- Lymph node metastasis: The prognostic role of regional lymphatic metastasis is controversial. There is evidence to support that regional lymph node metastases do not affect recurrence or survival. There is also evidence to support that lymph node metastases are a high risk factor for local recurrence and cancer-related mortality. There is a correlation between lymphatic metastases and distant metastases, especially those with bilateral cervical lymph node metastases, or extraperitoneal invasion of lymph nodes, or mediastinal lymph node metastases.
- Distant metastases: In DTC, distant metastases are a major cause of death. Approximately 10
 of PTC, 25 < img class="wp-image-30334" src="https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225908-word-image-1.png" /> of FTC will develop distant metastases. Distant metastases in eosinophilic glands
of PTC, 25 < img class="wp-image-30334" src="https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225908-word-image-1.png" /> of FTC will develop distant metastases. Distant metastases in eosinophilic glands - Surgical treatment of differentiated thyroid cancer
- Management of the primary focus: lesions with a T grade of T1 or T2, which are mostly confined to one lobe, are recommended for resection of the affected lobe and isthmus. For some patients with high-risk factors, total thyroidectomy is also indicated. These risk factors include multifocal cancer, lymph node metastases, distant metastases, family history, and early childhood exposure to ionizing radiation. Total thyroidectomy is also indicated in some cases where postoperative nuclear therapy is considered necessary. For tumors located in the isthmus, extended isthmus resection is indicated for smaller tumors, while total thyroidectomy may be considered for larger tumors or those with lymph node metastases.
- Medium-risk stratification
- The 2015 ATA Guidelines strongly recommend 131I therapy for patients stratified for high risk of recurrence
- 131I therapy may be considered for patients in intermediate-risk stratification with microscopic thyroid exenteration
- 131I therapy is not recommended in low-risk groups with ≤5 lymph node involvement (no extra-pericyclic invasion, lesions <0.2 cm). To facilitate follow-up by monitoring serum Tg levels and 131I whole-body imaging, 131I thyroid clearance therapy is feasible.
- Women during pregnancy or lactation.
- People who are planning a pregnancy within 6 months.
- Recommended 30mCi for thyroid clearance therapy in intermediate- and low-risk patients.
- For intermediate- and high-risk patients with suspected or proven microscopic residual disease or highly aggressive histologic subtypes (hypercellular, columnar cell, etc.) without distant metastases, an adjuvant 131I dose of 150 mCi is recommended.
- A higher dose of 131I is considered for patients with more residual thyroid tissue or focal clearance after incomplete/near-total thyroidectomy
- Thyroid clearance should be combined with focal clearance therapy at a 131I dose of 100-200 mCi in patients with residual surgically unresected DTC tissue in the neck, with inoperable or patient-refused cervical lymph nodes or distant metastases, and with unexplained elevated serum Tg levels after total thyroidectomy, especially irritant Tg. For adolescents, women of childbearing age, elderly patients, and. The dose of 131I may be reduced as appropriate in patients with mild to moderate renal impairment.
- For high-risk patients, an initial TSH target value of <0.1 mU/L is recommended.
- For intermediate-risk patients, an initial TSH target of 0.1 to 0.5 mU/L is recommended.
- For low-risk patients with undetectable serum Tg, a TSH target of 0.5 to 2 mU/L is recommended, regardless of whether 131I thyroid clearance therapy has been administered.
- For low-risk patients with undetectable serum Tg, a TSH target of 0.5 to 2 mU/L is recommended.
- For low-risk patients who have had 131I thyroid clearance and have low Tg levels or for low-risk patients who have not had 131I thyroid clearance and have slightly higher Tg levels, a TSH target of 0.1 to 0.5 mU/L is recommended;
- For low-risk patients who have had 131I thyroid clearance and have low Tg levels, a TSH target of 0.1 to 0.5 mU/L is recommended.
- For patients with lobectomy, a TSH target of 0.5 to 2 mU/L is recommended.
- For patients with an unsatisfactory outcome on imaging assessment, a TSH target of <0.1 mU/L is recommended in the absence of specific contraindications.
- For patients with an unsatisfactory outcome on imaging assessment, a TSH target of <0.1 mU/L is recommended in the absence of specific contraindications.
- For patients with unsatisfactory efficacy on serologic assessment, a TSH target of 0.1 to 0.5 mU/L is recommended based on initial ATA risk stratification, Tg levels, trends in Tg changes, and adverse effects of TSH suppressive therapy.
- For patients initially rated as high risk but with a satisfactory treatment response (clinical or serologic disease-free status) or unclear efficacy, a TSH target of 0.1 to 0.5 mU/L for up to 5 years with subsequent reduction in TSH suppression is recommended.
- For patients with a satisfactory treatment response (clinical or serologic disease-free status) or unclear efficacy, particularly those at low risk of relapse, a TSH target of 0.5 to 2 mU/L is recommended.
- For patients without 131I thyroid clearance or adjuvant therapy and with satisfactory or unclear outcome, meeting a negative neck ultrasound, low or undetectable suppressive Tg, and no trend toward increased Tg or TgAb, a TSH target of 0.5 to 2 mU/L is recommended.
- For the treatment of pulmonary metastases where the lesion is still iodine uptake and appears clinically effective, every
- For bone metastases, the dose is 100 to 200 mCi.
- Surgery or stereotactic external radiotherapy is recommended as the first consideration for central nervous system metastases.
- Continue TSH suppression therapy with close follow-up for patients with sTg <10 ng/ml from discontinuation of L-T4 or sTg <5 ng/ml from application of rhTSH, but empiric 131I therapy is feasible if there is a progressive increase in serum Tg or other evidence of disease progression (PD).
- For patients with sTg >10ng/ml from discontinuation of L-T4 or sTg >5ng/ml from rhTSH application, with persistently elevated Tg or TgAb levels and negative neck and chest imaging, 18F-FDG PET-CT, empiric 131I treatment at 100-200mCi is feasible, but if Rx-WBS is still negative However, if Rx-WBS remains negative, the patient is classified as iodine-refractory DTC and 131I therapy needs to be discontinued.
- Figure 3. Indications for radiotherapy for MTC
- Intensity-modulated radiation therapy (IMRT) and 3D conformal radiotherapy:
- Simulated CT localization:
- Target area development (Figure 4): there is considerable controversy regarding target area determination. Some studies suggest that small-field treatment can be used, with adequate attention to surgeons for external radiation to areas of high postoperative incidence and areas that are not easily resected surgically. Some investigators believe that large-field radiation should be used, with the option of treating areas of cervical lymph node drainage.
- High-risk area (CTV1): includes the thyroid area, surrounding lymph node drainage areas, and all areas with pathologically confirmed positive lymph nodes.
- Selective treatment area (CTV2): includes areas of lymph node drainage II-VI and upper mediastinal lymph nodes without pathologic confirmation but with potential metastasis, with a lower rate of metastasis in the retropharyngeal lymph nodes and in area I. However, the probability of metastasis in the retropharyngeal lymph nodes increases significantly if there are lymph nodes in area II, and the probability of metastasis in area Ib is increased if there are large lymph nodes in area IIa
- Localization: The same body position as for IMRT is recommended, using a simulated CT for localization and outlining the field on the planning system. Without analog CT equipment, X-ray orthogonal images can be used to outline the field.
- Radiographic field design:
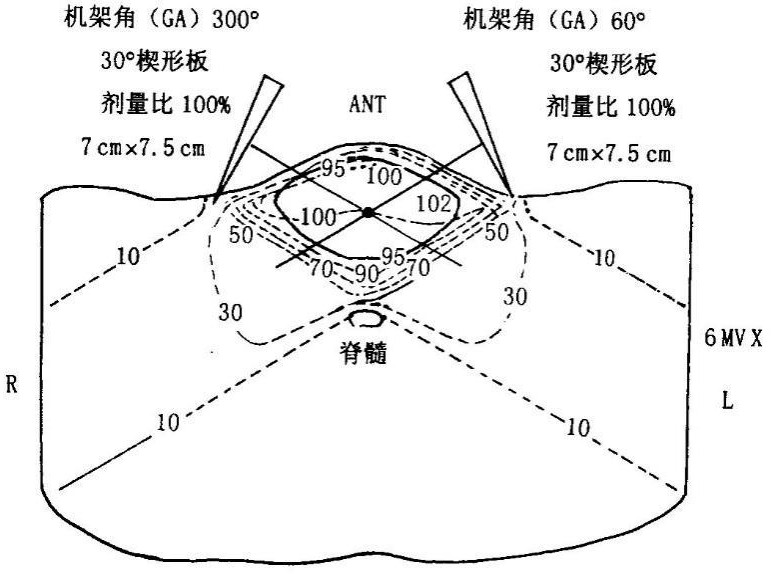 Two anterior oblique field cross-angle wedge Illumination technique: see Figure 6.
Two anterior oblique field cross-angle wedge Illumination technique: see Figure 6.- Irradiation dose: according to the radiotherapy protocol (macro-segmentation protocol and conventional segmentation radiotherapy prescription
- Acute complications: 1 to 2 degree reactions are more common in about 80
 or more, including pharyngitis, mucositis, dry mouth, taste changes, dysphagia, painful swallowing, radiolucent skin
or more, including pharyngitis, mucositis, dry mouth, taste changes, dysphagia, painful swallowing, radiolucent skin - Zheng Qi deficiency
- Liver and kidney deficiency
- Liver depression and qi stagnation
- For patients with distant metastatic high-risk differentiated thyroid cancer, surgery + postoperative 131I therapy + postoperative TSH suppression is the primary combination treatment modality.
- For localized lesions that are not surgically resectable, local radiofrequency ablation or external radiotherapy may be considered.
- The treatment of MTC should be primarily surgical, without TSH suppression, but with thyroxine replacement therapy.
- For ATC, external radiotherapy + surgery is preferred in the absence of distant metastases and airway obstruction
- For patients with DTC who have had total thyroid clearance (after surgery + 131I thyroid clearance), serum Tg levels should be measured regularly (along with TgAb), and the same test reagents are recommended. Long-term follow-up of serum Tg begins 6 months after 131I thyroid clearance therapy, when basal Tg or sTg is measured. sTg is repeated 12 months after 131I therapy, and basal Tg is repeated every 6 to 12 months thereafter. sTg may be repeated 3 years after thyroid clearance therapy for those at intermediate or high risk of recurrence.
- Neck ultrasound should be performed periodically during DTC follow-up to assess the status of the thyroid bed and lymph nodes in the central and lateral cervical regions of the neck. The first postoperative ultrasound examination is recommended 3 months after surgery in high-risk patients and 6 months after surgery in intermediate- and low-risk patients. If suspicious lesions are found, the examination interval can be shortened as appropriate. Ultrasound-guided puncture biopsy and/or Tg testing of the puncture eluate is indicated for suspicious lymph nodes.
- Patients with DTC may be followed up with Dx-WBS optionally after surgery and 131I thyroid clearance, depending on the risk of recurrence.
- 18F-FDG PET is not currently recommended for routine use in DTC follow-up, but may be considered in the following situations: (1) to assist in finding and localizing the lesion when serum Tg levels are elevated (>10 ng/ml) and Dx-WBS is negative; (2) to evaluate and monitor the disease in those with lesions that do not uptake iodine; and (3) to evaluate and monitor the disease in invasive or metastatic DTC.
- Long-term follow-up of DTC should also include the following: (1) long-term safety of 131I therapy: including effects on secondary tumors, reproductive system. However, over-screening and screening should be avoided; (ii) the effect of TSH suppression therapy: including whether TSH suppression therapy is achieved and the side effects of therapy; (iii) concomitant diseases in DTC patients: because some concomitant diseases (e.g., cardiac disease, other malignancies, etc.) may be of higher clinical urgency than DTC itself, the condition of these concomitant diseases should also be dynamically observed during long-term follow-up.
)peroxidaseantibodies (TPOAb) and TSH receptor antibodies (thyrotropin receptor antibody (TRAb)). In patients with DTC, TgAb is a thyroglobulin
(thyroglobulin, Tg) is an important ancillary test. Serum Tg levels are also affected by TgAb levels, which, when present, reduce the value of the chemiluminescent immunoassay for serum Tg and affect the accuracy of monitoring the disease by Tg. The presence of TPOAb, a key enzyme in the synthesis of thyroid hormones, usually precedes thyroid dysfunction and is involved in the tissue destruction process in the development of Hashimoto’s thyroiditis and atrophic thyroiditis, causing clinical symptoms of hypothyroidism. A positive TRAb test result indicates the presence of autoantibodies against the TSH receptor.
(3) Thyroid cancer tumor marker tests: thyroglobulin (Tg)
(Tg is a specific protein produced by the thyroid gland, but serum Tg measurement lacks specific value in identifying benign and malignant thyroid nodules. Therefore, serum Tg is not used for the preoperative diagnosis of DTC, but in the post-treatment follow-up period, serum Tg is an important tool to identify whether the patient has tumor recurrence, and can be used to monitor recurrence and metastasis after DTC. For patients with DTC who have removed all thyroid tissue, elevated serum Tg indicates the possibility of tumor recurrence and should be further examined. For patients with DTC without complete thyroid removal, it is still recommended to measure serum Tg periodically (every 6 months) after surgery, and for those with persistently elevated serum Tg levels after surgery, thyroid tissue or tumor growth should be considered and further evaluation is needed in combination with other tests such as neck ultrasound.
Serum Tg measurement in DTC follow-up includes basal Tg measurement (in TSH suppressed state) and Tg measurement after TSH stimulation (TSH > 30 mU/L). To more accurately reflect the condition, serum TSH levels can be increased to >30 mU/L by discontinuing L-T4 or applying recombinant human thyrotropin (rhTSH), followed by Tg measurement after TSH stimulation, i.e., post-TSH stimulation Tg measurement. Tg levels measured after discontinuation of L-T4 and use of rhTSH were highly concordant. Patients with DTC stratified as intermediate or high risk of recurrence may be tested for post-TSH stimulation Tg if necessary. It should be noted that Tg should be tested at the same time as TgAb. If TgAb is elevated, it is not possible to determine the presence of DTC by
Tg to determine the presence or absence of recurrence of DTC. If DTC cells are poorly differentiated, unable to synthesize and secrete Tg or produce defective Tg, follow-up with Tg is also not possible. The sensitivity of detecting lymph node metastases in DTC can be improved by measuring Tg levels in lymph node puncture needle eluate for lymph nodes that are palpable on examination and for suspicious cervical lymph nodes detected by ultrasound.
Patients with MTC are recommended to have both serum calcitonin and CEA measured prior to treatment and to monitor serum levels periodically after treatment. If serum calcitonin exceeds the normal range and continues to increase, especially if calcitonin is ≥150 pg/ml, progression or recurrence should be highly suspected. Serum calcitonin and CEA tests are useful for the assessment of efficacy and monitoring of the disease in patients with myeloid carcinoma.
(4) Relevant molecular tests for diagnosis: for thyroid nodules whose benignity or malignancy cannot be determined by fine-needle aspiration (FNA), molecular markers such as BRAF mutation, RAS mutation and RET/PTC rearrangement can be tested on the puncture specimens, which can help to improve the diagnosis rate. The detection of BRAF mutations in preoperative puncture specimens can also help in the diagnosis and clinical prognosis of papillary thyroid cancer and facilitate the development of individualized diagnosis and treatment plans.
(iv) Imaging.
- Ultrasonography
This refers to an increase in nodule volume of more than 50  or At least 2 diameter lines increase by more than 20
or At least 2 diameter lines increase by more than 20  (and more than 2 mm), then there is an indication for FNAB; for cystic nodules, the decision to perform FNAB should be based on the growth of the solid portion.
(and more than 2 mm), then there is an indication for FNAB; for cystic nodules, the decision to perform FNAB should be based on the growth of the solid portion.
In postoperative thyroid patients, attention should be paid to the presence of solid lesions in the operative bed and to the presence of malignant cervical lymph nodes during follow-up. Ultrasound is difficult to identify benign lesions and recurrent lesions in the operative bed, and the evaluation of cervical lymph nodes is the same as preoperatively. The indications for postoperative puncture of suspicious cervical lymph nodes: for lymph nodes with a minimum diameter greater than 8mm and abnormal ultrasound, cytology of fine needle puncture material + eluate for Tg level can be considered; for lymph nodes smaller than 8 mm, follow-up can be performed if they do not grow or threaten the surrounding important structures.
The normal thyroid gland contains high iodine content and has a significantly different density from the surrounding tissues, which can be clearly visualized by CT plain scan, with even better contrast after contrast injection. CT scan is of great value in evaluating the extent of the thyroid tumor, its relationship with important surrounding structures such as trachea, esophagus, carotid artery and the presence of lymph node metastasis. CT has the advantage of observing the central group of lymph nodes, the upper mediastinal group of lymph nodes and the posterior pharyngeal group of lymph nodes, and can observe the posterior sternal thyroid lesions, larger lesions and their relationship with the surrounding structures, and can clearly show calcified foci of various shapes and sizes, but for nodules with a maximum diameter of ≤5 mm and However, it is not good for patients with diffuse lesions combined with nodules. For recurrent thyroid cancer, CT can provide information about the residual thyroid gland, assess the location of the lesion and its relationship with the surrounding tissues, evaluate the size and location of metastatic lymph nodes, and assess the presence of pulmonary metastases. If there is no contraindication to the use of iodine contrast.
Enhanced scans should be routinely performed for thyroid lesions. Thin layer images can reveal smaller lesions and clearly show the relationship of the lesion to surrounding tissues and organs.
The high tissue resolution allows for multi-directional and multi-parametric imaging to evaluate the extent of the lesion and its relationship to surrounding vital structures. Dynamic enhancement scans, diffusion-weighted imaging, and other functional imaging can be used to assess the benignity and malignancy of nodules. The shortcomings of MRI include insensitivity to calcification, long examination time, and susceptibility to breathing and swallowing movements.
Positron emission tomography-computed tomography (PET-CT) is not recommended as a routine test for the diagnosis of thyroid cancer, but may be considered in the following cases, if available: 1) elevated Tg (>10ng/ml) at follow-up in patients with DTC and iodine -131 (131I) diagnostic whole body scan (Dx-WBS) is negative to detect metastases.
(2) Pre-MTC staging and post-operative calcitonin elevation for metastases; (3) Pre-MTC staging and post-operative follow-up for undifferentiated thyroid cancer; (4) Pre-131I evaluation for patients with invasive or metastatic DTC (lesions showing increased PET-CT metabolism have poor iodine uptake and may not benefit from 131I therapy).
(v) Vocal fold function assessment.
Patients with thyroid cancer should be routinely evaluated for bilateral vocal fold activity preoperatively. Laryngoscopy (indirect laryngoscopy or fiberoptic laryngoscopy) can be performed. If signs of reduced or even fixed vocal fold activity are present, tumor compression or invasion of the recurrent laryngeal nerve should be highly suspected, which helps to assess the condition and surgical risk. In addition, for patients with clinical or imaging examinations (e.g., CT of the neck) suspecting tumor adjacent to or invading the trachea, preoperative fiberoptic bronchoscopy should be performed to assess whether the tumor invades the whole layer of the trachea to the tracheal lumen, as well as the extent of invasion and whether it affects the anesthetic tracheal intubation, etc., so as to formulate the corresponding surgical plan and anesthetic plan.
If tumor invasion of the recurrent laryngeal nerve is detected intraoperatively, or if intraoperative recurrent laryngeal nerve monitoring indicates that recurrent laryngeal nerve function is compromised, laryngoscopic assessment of vocal fold motor recovery is indicated postoperatively. In patients who have undergone tracheostomy or tracheotomy because of bilateral invasion of the laryngeal nerve, laryngoscopic assessment of vocal fold motion is indicated to determine the timing of removal of the tracheal tube or tracheostomy repair.
(vi) Pathology.
The cytopathologic diagnostic guidelines for thyroid cancer consist of sections on the sampling, production, and diagnostic reporting of thyroid FNA.
and a needle with an outer diameter of 5 to 5 G.FNA can be performed with a small amount of negative pressure or without negative pressure, and the needle should be performed in multiple angles and quickly. The number of needle insertions per nodule is 1 to 3, depending on the amount of needle aspiration. For cystic nodules there should be a targeted extraction of the solid zone.
- FNA production
(Table 3)
(Table 3).
Table 2 TBSRTC diagnostic grading criteria
I Non-diagnostic/unsatisfactory cyst fluid specimen
Low amount of epithelial cells
Other (e.g., blood much obscuring cells, excessive cell dryness, etc.) Ⅱ Benign
Consistent with benign follicular nodules (including adenomatous nodules and glial nodules, etc.) Consistent with Hashimoto’s thyroiditis
Consistent with subacute thyroiditis
III Atypical cells of undetermined significance/follicular lesions of undetermined significance IV Follicular neoplasm/suspected follicular neoplasm
If eosinophilic tumor, specify V Suspicious malignant
Suspected papillary thyroid carcinoma Suspected medullary thyroid carcinoma Suspected metastatic carcinoma
Suspected lymphoma VI Malignant
Papillary carcinoma of thyroid Hypofractionated carcinoma of thyroid Medullary carcinoma of thyroid Undifferentiated carcinoma of thyroid Squamous cell carcinoma
Carcinoma of mixed components (specify specific components) Metastatic malignancy
Non-Hodgkin’s lymphoma other
 Table 3 Malignant risk and clinical management of TBSRTC by diagnostic classification
Table 3 Malignant risk and clinical management of TBSRTC by diagnostic classification
 ~10
~10 


>
Follicular neoplasm/suspicious follicular



>

 Histopathologic Diagnostic Guidelines for Thyroid Cancer
Histopathologic Diagnostic Guidelines for Thyroid Cancer
In order to better assist clinicians in making accurate diagnosis and treatment plans, it is important to standardize thyroid histopathology so that different levels of hospitals and different pathologists can be on the same platform to communicate with each other about patient care.
.
Notes for sending frozen pathology include.
(1) Thyroid: (1) Send the specimen to the pathology department as soon as possible after isolation without any fixative.
②If the tumor nodule is <5 mm, markings (e.g., incision or tied sutures) at the tumor may be considered.
③The diagnosis of follicular thyroid tumors, including junctional tumors and follicular carcinoma, requires postoperative observation of the specimen as a whole and adequate sampling to confirm the diagnosis. (2) Lymph nodes: ①Separate the lymph nodes for examination to increase the purpose of the subdivision and the accuracy of the pathological diagnosis.
(2) Lymph nodes: ①Separate the lymph nodes for examination to increase the purpose and accuracy of pathological diagnosis. ②Send the specimens as soon as possible after isolation, keep them fresh, put them in transparent plastic pouches or specimen boxes, seal them well, and send them to the pathology department. ③The too-small specimen should not be left outside the body for too long to avoid drying and hardening, resulting in inability to freeze the film or accurate observation under the microscope. ④If sand granules are found in the lymph nodes under the pathology microscope, they should be
serial sections to look for evidence of metastasis or not. ⑤ It is not uncommon for lymph nodes to be negative for intraoperative freezing and metastatic cancer to appear in deep postoperative paraffin cuts, which needs to be informed to the patient and family as informed consent and signed before surgery or freezing.
.(vii) lymph node metastasis + extra-peritoneal invasion of lymph nodes; (viii) pTNM staging (AJCC 8th edition); (ix) immunohistochemistry as necessary.
(vii) Differential diagnosis.
III.
(A) Histologic classification of thyroid cancer.
According to the WHO definition, the histologic classification of thyroid tumors is mainly divided into primary epithelial tumors, primary non-epithelial tumors, and secondary tumors. The specific classification is shown in Table 4.
Table 4 Histologic classification of WHO thyroid tumors
Cross-sectional: Follicular tumors of undetermined malignant potential, highly differentiated tumors of undetermined malignant potential, noninvasive follicular tumors with papillary nuclei, and hyaline metachronous tumors.
Malignant: Thyroid cancer, including ① Differentiated thyroid cancer: PTC, FTC, eosinophilic carcinoma.
FTC, eosinophilic carcinoma; ②PDTC; ③ATC.
The thyroid has two different endocrine cells with different functions. About 95  of thyroid tumors arise from The rest are mostly derived from parafollicular cells of the thyroid. Mixed follicular epithelial and parafollicular cell tumors are rare, and tumor cells containing both follicular epithelial and parafollicular cell sources are of histologic origin as a
of thyroid tumors arise from The rest are mostly derived from parafollicular cells of the thyroid. Mixed follicular epithelial and parafollicular cell tumors are rare, and tumor cells containing both follicular epithelial and parafollicular cell sources are of histologic origin as a
The histologic origin of this tumor as a separate thyroid tumor is controversial. Thyroid lymphoma is the most common tumor of non-epithelial origin of the thyroid gland and may occur independently of the thyroid gland or as part of a systemic lymphatic tumor. Thyroid sarcomas and secondary thyroid malignancies are less common in clinical practice.
PTC is the most common malignant epithelial tumor of follicular epithelial origin with characteristic PTC nuclear features. The classic PTC has two basic morphologic features: papillary and infiltrative/PTC nuclear features, with rare nuclear schwannomas and more common sandy calcifications, mainly in the lymphatic vessels or interstitium. The literature reports that 20  to 40
to 40  squamous metaplasia is seen in 20 to 40 cases. Lymphovascular invasion is common; vascular invasion is uncommon but can occur. Immunophenotype: TG, TTF1, PAX8, and broad-spectrum CK positive; CK20, CT, and neuroendocrine markers usually negative. The follicular subtype accounts for approximately 40% of PTC
squamous metaplasia is seen in 20 to 40 cases. Lymphovascular invasion is common; vascular invasion is uncommon but can occur. Immunophenotype: TG, TTF1, PAX8, and broad-spectrum CK positive; CK20, CT, and neuroendocrine markers usually negative. The follicular subtype accounts for approximately 40% of PTC  , with a predominantly follicular growth pattern. The predominantly follicular growth pattern has the karyotype of classic PTC.
, with a predominantly follicular growth pattern. The predominantly follicular growth pattern has the karyotype of classic PTC.
There are 14 subtypes of PTC, including micro PTC, encapsulated, follicular, diffuse sclerosing, sieve-mulberry, hypercellular, columnar cell, bootstrap, solid/beam, eosinophilic, worsinoma-like, clear cell, spindle cell, and papillary carcinoma with fibromatosis/fasciitis-like interstitium. The hypercellular, spike, columnar cell, and solid types are generally considered to be invasive PTCs with relatively complex genotypes and a poorer prognosis than classic types.
- Diffuse sclerosis: Most often seen in young women with diffuse bilateral or unilateral enlargement of the thyroid lobes with the serologic features of autoimmune thyroiditis. Morphologic features commonly include marked sclerosis, numerous gravelly bodies, a background of chronic lymphocytic thyroiditis, and often solid nests of tumor cells with extensive squamous metaplasia that readily invade the intrathyroidal lymph nodes
The tumor nests are often solid, with extensive squamous metaplasia, and tend to invade the intrathyroidal lymphatic ducts and extrathyroidal tissue. Molecular detection of RET rearrangements is common, while BARF mutations are rare. About 10  to 15
to 15  distant metastases occur in about 10 of cases, most commonly to the lung. . Disease-free survival is shorter, but mortality is not significantly different from the common type.
distant metastases occur in about 10 of cases, most commonly to the lung. . Disease-free survival is shorter, but mortality is not significantly different from the common type.
- High cell subtype: ≥30
 Cancer cells are more than 2 to 3 times as tall as they are wide, with abundant eosinophilic cytoplasm and typical PTC karyotype, often in single rows or parallel arrangements. It is more aggressive than classic type and more likely to have extrathyroidal invasion and distant metastasis. Most cases have a BRAF mutation (60
Cancer cells are more than 2 to 3 times as tall as they are wide, with abundant eosinophilic cytoplasm and typical PTC karyotype, often in single rows or parallel arrangements. It is more aggressive than classic type and more likely to have extrathyroidal invasion and distant metastasis. Most cases have a BRAF mutation (60  to 95
to 95  ).
).
.
but does not express p63, TG, TTF1, ER, β-linked proteins, and CK19.
FTC is a malignant tumor of follicular cell origin of the thyroid gland that lacks the nuclear features of papillary carcinoma, usually has an envelope, and has an infiltrative growth pattern. Incidence 6  to 10
to 10  . Subtypes include.
. Subtypes include.
(1) follicular carcinoma, microinfiltrative (envelope invasion only); (2) follicular carcinoma, intraenvelope vascular infiltration; (3) follicular carcinoma, extensive infiltration. lymph node metastasis is less common in FTC than in PTC and is more likely to occur distantly. common mutations in FTC include RAS point mutations, PAX8-PPARG fusions, TERT promoter mutations, etc. BRAF mutations and RET fusions are uncommon. BRAF mutations and RET fusions are uncommon.
Hürthle cell tumors are a group of tumors with 75 
Hürthle cell adenoma (eosinophilic adenoma) and Hürthle cell carcinoma (eosinophilic carcinoma).
3.
MTC is a malignant tumor of parafollicular cell (follicular cell) origin of the thyroid gland. Incidence 2  ~3
~3  , sporadic and familial, sporadic accounting for about 70% of all myeloid carcinomas . The sporadic form accounts for about 70% of all medullary carcinomas
, sporadic and familial, sporadic accounting for about 70% of all myeloid carcinomas . The sporadic form accounts for about 70% of all medullary carcinomas  and is more common in the The age group of 50 to 60 years old, with familial incidence at a younger age, accounts for about 30
and is more common in the The age group of 50 to 60 years old, with familial incidence at a younger age, accounts for about 30 
The microscopic morphology of MTC is diverse and can resemble any thyroid malignancy, with typical structures being solid, lobulated, tubular or insular. The tumor cells are highly variable in size and can be round, polygonal, plasma cell-like, or spindle-shaped. The nuclei are low-moderate heterogeneous and have relatively low nuclear fission activity.
Subtypes: There are different types based on cellular and structural features, papillary/pseudopapillary, follicular (ductal/glandular), spindle cell, giant cell, clear cell, eosinophilic, melanotic, squamous subtype, paraganglioma-like, angiosarcoma-like, small cell, and intraepithelial medullary thyroid carcinoma.
Immunohistochemical indicators: calcitonin, neuroendocrine markers (CD56, synaptophysin, chromogranin A), TTF-1, PAX8 and CEA can be expressed; TG is not expressed.
4.
PDTC are malignant tumors showing limited follicular cell differentiation and are intermediate in morphology and biological behavior between DTC and ATC. The main histological patterns are insular, beam-like and solid.
PDTC can be accompanied by varying proportions of differentiated carcinoma components, but some studies have shown that even in the presence of 10  of PDTC components are accompanied by aggressive behavior and poor prognosis. The Ki-67 index of PDTC usually ranges from 10
of PDTC components are accompanied by aggressive behavior and poor prognosis. The Ki-67 index of PDTC usually ranges from 10 
 , and the Ki-67 index of PDTC is usually between 10
, and the Ki-67 index of PDTC is usually between 10  to 40
to 40  Patients with distant metastases such as lung, bone and brain. The main histologic patterns are sarcomatoid, tumor giant cell-like, and epithelioid, which may occur alone or in different proportions, or with focal squamous differentiation or heterologous differentiation; usually accompanied by necrosis, numerous nuclear schwannomas, and vascular invasion. Immunohistochemistry: TTF1 and TG are usually negative, PAX8 is positive in approximately half of cases, CK can be positive in areas of epithelioid differentiation, and LCA, myogenic markers, and melanoma markers are mainly used for exclusionary diagnosis. Differential diagnosis: other types of highly malignant tumors such as myogenic sarcoma, malignant melanoma, and large cell lymphoma. Highly malignant primary thyroid tumors of non-follicular and parafollicular cell origin are also generally classified as ATC, such as squamous cell carcinoma, sarcoma, mucinous epidermoid carcinoma, and others.
Patients with distant metastases such as lung, bone and brain. The main histologic patterns are sarcomatoid, tumor giant cell-like, and epithelioid, which may occur alone or in different proportions, or with focal squamous differentiation or heterologous differentiation; usually accompanied by necrosis, numerous nuclear schwannomas, and vascular invasion. Immunohistochemistry: TTF1 and TG are usually negative, PAX8 is positive in approximately half of cases, CK can be positive in areas of epithelioid differentiation, and LCA, myogenic markers, and melanoma markers are mainly used for exclusionary diagnosis. Differential diagnosis: other types of highly malignant tumors such as myogenic sarcoma, malignant melanoma, and large cell lymphoma. Highly malignant primary thyroid tumors of non-follicular and parafollicular cell origin are also generally classified as ATC, such as squamous cell carcinoma, sarcoma, mucinous epidermoid carcinoma, and others.
(b) Staging of thyroid cancer.
Clinical staging can be established based on preoperative assessment (history, physical examination, ancillary tests)
(cTNM). Pathologic staging (pTNM) was obtained based on postoperative pathologic findings. The specific staging criteria are shown in Tables 5 and 6 (AJCC 8th edition).
Table 5 Definition of TNM staging
carcinoma
organs and soft tissues such as larynx, trachea, esophagus, laryngeal denervation and subcutaneous soft tissues
artery, mediastinal vessels
or upper mediastinum) lymph nodes, either unilaterally or bilaterally
III, IV, or V areas) or retropharyngeal lymph node metastases
Table 6 TNM staging of thyroid cancer
Period
Period
Period
Period
Period
Period
Period
stage
Period
Period
Period
Period
stage
Period
A number of characteristics of the tumor will affect the prognosis of the tumor. Some of the more important factors include tissue type, primary tumor size, extraglandular invasion, vascular infiltration, BRAF mutations, and distant metastases.
- Tissue type: Survival rates for patients with PTC are generally good, but tumor mortality varies widely between specific subtypes. Among these, the hypercellular, shoe-peg, columnar cell, and solid types are the aggressive subtypes.
FTC is typically characterized by isolated tumors with an envelope and is more aggressive than PTC. fTC usually has microfollicular structures and is diagnosed as carcinoma because of infiltration of follicular cells into the envelope or blood vessels. the prognosis is worse for those with infiltration into blood vessels than for those with infiltration into the envelope. Highly invasive FTCs are uncommon and are often seen to invade surrounding tissues and blood vessels intraoperatively. Approximately 80  of highly invasive FTCs will distant metastases, which can lead to about 20
of highly invasive FTCs will distant metastases, which can lead to about 20  of patients die within a few years of diagnosis. Poor prognosis is strongly associated with older age, higher tumor stage, and larger tumor size at the time of diagnosis.
of patients die within a few years of diagnosis. Poor prognosis is strongly associated with older age, higher tumor stage, and larger tumor size at the time of diagnosis.
PTC has a similar prognosis to FTC, with both having a better prognosis if the tumor is confined to the thyroid, is less than 1 cm in diameter, or is minimally metastatic. If distant metastases and high invasiveness are present, the prognosis is poor.
- Primary tumor size: Papillary carcinoma <1 cm, called microscopic carcinoma, is usually detected on physical examination and has an almost zero lethality rate and a low risk of recurrence. However, microscopic cancer is not always a tumor with a low risk of recurrence. For example, about 20
 of multifocal microscopic cancers There is also a risk of distant metastasis.
of multifocal microscopic cancers There is also a risk of distant metastasis.
The size of the primary tumor is associated with prognosis and mortality. It has been shown that DTC with primary tumors <1.5 cm in maximum diameter are less likely to develop distant metastases, while larger tumors (>1.5 cm) have a recurrence rate of approximately 33% within 30 years  . The 30-year mortality rate of DTC with a maximum diameter <1.5cm is 0.4
. The 30-year mortality rate of DTC with a maximum diameter <1.5cm is 0.4  and 7 for larger tumors (>1.5 cm)
and 7 for larger tumors (>1.5 cm)  .
.
- Local invasion: approximately 10
 of DTC invade surrounding organs/structures, and the local recurrence rate is approximately twice that of non-invasive tumors. Patients with invasive cancer also have elevated mortality, with approximately 1 in 3 patients dying.
of DTC invade surrounding organs/structures, and the local recurrence rate is approximately twice that of non-invasive tumors. Patients with invasive cancer also have elevated mortality, with approximately 1 in 3 patients dying.
cancer and in patients >40 years of age (35  ). The most common location of distant metastases is the lung, followed by bone, liver, and brain. Distant metastases make the prognosis worse.
). The most common location of distant metastases is the lung, followed by bone, liver, and brain. Distant metastases make the prognosis worse.
The overall prognosis of DTC is good, with relatively low mortality. However, disease recurrence rates vary widely depending on clinicopathologic features. Patients were classified into 3 strata of risk of recurrence based on intraoperative pathologic features such as residual lesions, tumor size and number, pathologic subtypes, envelope vascular invasion, lymph node metastasis and extravasation, postoperative Tg levels after TSH stimulation (sTg), and molecular pathologic features (Table 7). Postoperative adjuvant therapy is strongly recommended for DTC in the high-risk group; adjuvant therapy can be considered in the intermediate-risk group; 131I thyroid clearance is generally not indicated in the low-risk group, but endocrine therapy should be considered.
Table 7 Clinicopathologic features of DTC recurrence risk stratification
No residual tumor without extranodal invasion of the bulk of the tumor
Non-malignant histologic subtype
No iodine uptake foci outside the thyroid bed without vascular invasion on first post-operative whole-body nuclide scan
cN0 or less than 5 small lymph node metastases (<0.2 cm in diameter)
Follicular subtype PTC, located within the thyroid, not breaching the envelope; tiny thyroid papillae
FTC, located in the thyroid gland, well differentiated, with envelope invasion and no vascular invasion, or only minimal vascular invasion
Microinvasion of peri-thyroidal tissue
first postoperative nuclear imaging with iodine uptake in the neck lesion
Highly malignant subtype (hypercellular, columnar cell, diffuse sclerosis, etc.) with vascular invasion
cN1 or pN1 with more than 5 lymph node metastases and metastases less than 3 cm in diameter
Multifocal papillary microcarcinoma of the thyroid with or without BRAF V600E mutation
Obvious invasion of soft tissue tumor remnants around the thyroid
Distant metastasis
High postoperative serum Tg suggesting distant metastasis
pN1 and metastatic lymph node metastases ≥3 cm in diameter
Extensive vascular invasion of follicular thyroid cancer (>4 vascular invasions)
IV.
(a) Surgical treatment of thyroid cancer.
Treatment of DTC is primarily surgical, supplemented by postoperative endocrine therapy, radionuclide therapy, and in some cases, radiation therapy and targeted therapy. mtc is primarily surgical, supplemented in some cases by radiation therapy and targeted therapy. In the treatment of undifferentiated cancer, a few patients have the opportunity to undergo surgery, and some patients may have some effect with radiotherapy and chemotherapy, but the overall prognosis is very poor and survival time is short. However, the overall prognosis is very poor and survival time is short. It should also be noted that individualization of tumor treatment is very important, and each patient’s condition and demands are different, so there is some flexibility in clinical diagnosis and treatment.
A subset of T1 lesions are low-risk micro papillary carcinomas. Because of its relatively slow progression and low lethality, conservative therapy, which involves active surveillance and close follow-up, can be considered in addition to surgical treatment. Low-risk papillary carcinoma that can be closely monitored generally has the following characteristics: (1) the primary tumor is a single lesion, (2) the maximum diameter of the primary lesion is <1 cm, (3) the location of the primary lesion is located in the central part of the thyroid gland rather than immediately adjacent to the thyroid peritoneum or trachea, and (4) there are no regional lymph node metastases after evaluation. In addition to the above conditions, the patient should be considered for any history of high dose radiation exposure during early childhood, thyroid cancer, and the presence of a metastatic node.
In addition to the above, specific factors such as history of exposure to high doses of ionizing radiation during childhood, family history of thyroid cancer, and the presence of hyperthyroidism should be considered. If closely monitored, re-evaluation is usually required every 6 months. If the evaluation reveals progression of the primary tumor (e.g., 2-3 mm in diameter, new tumor lesions, or clinically suspicious metastatic regional lymph nodes), discontinuation of conservative treatment should be considered.
For T3 lesions with large tumors or those that have invaded the extraperitoneal muscles of the thyroid, total thyroidectomy is recommended. However, for lesions closer to the thyroid peritoneum, which may not be large per se but have invaded the extraperitoneal muscles, excision of the affected lobe and isthmus, together with excision of the invaded muscles, may be performed. The specific surgical options are recommended, weighing the benefits and risks of surgery.
For T4 lesions that have invaded the surrounding structures, total thyroidectomy is usually recommended; for T4a lesions, removal of the thyroid gland along with partial removal of the affected structures, such as part of the larynx (or even the whole larynx), part of the airways, and the larynx.
(T4b lesions are generally considered to be inoperable, but the possibility of surgery is determined on a case-by-case basis and may require multidisciplinary collaboration with vascular surgery, orthopedics, and neurosurgery. In general, however, T4b lesions are difficult to completely resect, have a poor prognosis, are associated with higher surgical risks, and have more postoperative complications. Surgical treatment requires careful evaluation of the condition, with a focus on whether the patient will benefit from surgery. Sometimes, palliative decompression therapy is necessary, such as a tracheotomy to relieve dyspnea.
- Management of regional lymph nodes: central zone lymph nodes (zone VI): cN1a The affected central zone should be cleared. If the lesion is on one side, it is recommended that the central zone be cleared to include the affected tracheoesophageal groove and the anterior trachea. The anterior laryngeal region is also part of the central zone sweep, but the anterior laryngeal gonad
The metastasis to the nodes is rare and can be individualized. For patients with cN0, central zone clearance may be considered in the presence of high-risk factors (e.g., T3 to T4 lesions, multifocal carcinoma, family history, history of early childhood ionizing radiation exposure). For low-risk patients with cN0 (without high-risk factors), the treatment can be individualized. The extent of central zone clearance is defined as the level of the superior border of the innominate artery at the inferior border, the level of the hyoid bone at the superior border, and the medial border of the common carotid artery at the lateral border, including the anterior trachea. The right tracheoesophageal groove requires attention to the lymphatic adipose tissue at the deep level where the laryngeal recurrent nerve is located. Central
If the parathyroid glands cannot be preserved in situ, parathyroid autotransplantation should be performed.
Lateral cervical lymph node dissection (zones I-V): Lateral cervical lymph node metastases are most often seen in zones III and IV, followed by zones II and V. Zone I is less common. Lateral cervical lymph node dissection is recommended for therapeutic dissection, i.e., lateral cervical dissection when N1b is confirmed by preoperative evaluation or intraoperative freezing. The recommended scope of lateral neck dissection includes zones II, III, IV, and VB, with zones IIA, III, and IV being the smallest. Zone I does not require routine clearance. The schematic diagram of the neck partition and the specific division of each zone are shown in Figure 1 and Table 8.
The parapharyngeal lymph nodes, upper mediastinal lymph nodes, and other special areas of lymph nodes are recommended for simultaneous surgical resection when metastasis is considered on imaging.
For MTC, total thyroidectomy is recommended. In the case of MTC diagnosed after lobectomy, a total thyroidectomy is recommended. In individual cases, sporadic microscopic MTC found incidentally after lobectomy may also be considered for close observation.
MTC is more prone to cervical lymph node metastases, and most patients have lymph node metastases at the time of presentation, so removal of the primary site should be accompanied by cervical lymph node dissection (central or lateral cervical area), the extent of which should be determined by serum calcitonin levels in addition to clinical evaluation.
Some MTCs are hereditary myeloid carcinomas and can be treated by detecting germline mutations in the RET gene.
(The diagnosis can be made by testing for germline mutations in the RET gene (by genetic testing of somatic cells or blood leukocytes). In this group, total thyroidectomy and cervical lymph node dissection are recommended. In the case of MEN II patients, the systemic situation should be evaluated. Pheochromocytoma, for example, needs to be managed before considering thyroid surgery.
A small number of patients with undifferentiated cancer have small tumors at the time of presentation and may have access to surgery. Most patients with undifferentiated cancer have a large and rapidly progressing neck mass at the time of presentation and have no chance of surgery. Tracheotomy can be considered when the tumor compresses the trachea and causes respiratory distress.
In addition to conventional rehydration, dexamethasone and neurotrophic drugs can be given as adjunctive therapy to reduce neuroedema after thyroid cancer surgery. In patients with total thyroidectomy, parathyroid hormone and blood calcium should be reviewed, and those with low calcium should be given calcium supplements and oral vitamin D and calcium as soon as they can eat. Patients with injury to one laryngeal nerve often choke on food and water during the acute phase. If necessary, a tracheotomy kit should be placed at the bedside. Patients with bilateral laryngeal return nerve injury are usually treated intraoperatively with a tracheal tube and postoperative care of the tracheotomy opening. For patients with cervical lymph node dissection, postoperative attention should be paid to the functional exercise of the neck and shoulder.
Postoperative care should be paid to the functional exercise of the neck and shoulder. A postoperative adjuvant treatment plan should be developed and communicated to the patient according to pathologic staging and risk stratification.
(b) Common postoperative complications.
Surgical complications are other surgically related conditions that occur during the surgical treatment of disease and have a certain probability of occurring and are not completely avoidable.
The incidence of postoperative bleeding in thyroid cancer is about 1  to 2
to 2  , mostly within 24 hours after surgery. The main manifestation is an increase in drainage, with a tendency to show an increase in flow. The main manifestations are increased, bloody drainage, swelling of the neck, and difficulty in breathing. If the drainage is >100 ml/h, active bleeding is considered and prompt debridement should be performed to stop the bleeding. If the patient is in respiratory distress, the airway should be controlled first, and the bedside incision can be opened in an emergency to relieve the pressure of the hematoma on the trachea first. Risk factors for postoperative bleeding in thyroid cancer include combined hypertension, anticoagulant medications, or aspirin.
, mostly within 24 hours after surgery. The main manifestation is an increase in drainage, with a tendency to show an increase in flow. The main manifestations are increased, bloody drainage, swelling of the neck, and difficulty in breathing. If the drainage is >100 ml/h, active bleeding is considered and prompt debridement should be performed to stop the bleeding. If the patient is in respiratory distress, the airway should be controlled first, and the bedside incision can be opened in an emergency to relieve the pressure of the hematoma on the trachea first. Risk factors for postoperative bleeding in thyroid cancer include combined hypertension, anticoagulant medications, or aspirin.
The incidence probability of laryngeal nerve injury in thyroid surgery is reported in the literature as 0.3  to 15.4
to 15.4 
Injury to the superior laryngeal nerve, the patient’s voice becomes muffled after surgery. Intraoperative management of the supraglottic artery should be performed with close dissection of the thyroid gland to reduce the probability of supraglottic nerve injury.
The intraoperative neuromonitoring (IONM) technique can help to localize the recurrent laryngeal nerve intraoperatively, to detect the function of the recurrent laryngeal nerve after the specimen is lowered, and to locate the injured segment if there is nerve damage. IONM is recommended for secondary surgery, large thyroid masses, and preoperative nerve palsy on one side, when available.
Fine dissection along the peritoneum, intraoperative exposure of the recurrent laryngeal nerve, proper use of energy instruments, and standard use of IONM can reduce the probability of nerve injury.
The incidence of postoperative permanent is about 2  ~15
~15  , mostly after total thyroid This is usually seen after total thyroid removal. The main manifestation is postoperative hypocalcemia, with patients experiencing tingling of the hands and feet, perioral numbness, or twitching of the hands and feet, which is relieved by intravenous calcium drips. For temporary hypoparathyroidism, calcium can be given to relieve the symptoms, with the addition of osteopontin if necessary. Prophylactic dosing may be considered to reduce postoperative symptoms. In permanent hypoparathyroidism, lifelong calcium and vitamin D supplements are required. Intraoperative attention should be paid to the fine dissection along the perineurium and to the protection of the blood supply when the parathyroid glands are preserved in situ. Some staining techniques can assist in the intraoperative identification of the parathyroid glands, such as nano-carbon negative contrast.
, mostly after total thyroid This is usually seen after total thyroid removal. The main manifestation is postoperative hypocalcemia, with patients experiencing tingling of the hands and feet, perioral numbness, or twitching of the hands and feet, which is relieved by intravenous calcium drips. For temporary hypoparathyroidism, calcium can be given to relieve the symptoms, with the addition of osteopontin if necessary. Prophylactic dosing may be considered to reduce postoperative symptoms. In permanent hypoparathyroidism, lifelong calcium and vitamin D supplements are required. Intraoperative attention should be paid to the fine dissection along the perineurium and to the protection of the blood supply when the parathyroid glands are preserved in situ. Some staining techniques can assist in the intraoperative identification of the parathyroid glands, such as nano-carbon negative contrast.
Thyroid surgery is mostly a type I incision, with a small number of type II incisions involving the larynx, trachea, and esophagus. The incidence of postoperative thyroid incision infection is approximately 1 
 . The risk of incisional infection
. The risk of incisional infection
Factors include cancer, diabetes, and immunocompromise. The signs of incisional infection include fever, cloudy drainage, redness and oozing of the incision, increased skin temperature, and local pain with pressure. If incisional infection is suspected, antibiotic treatment should be given promptly, and the incision should be opened and changed if there is abscess accumulation. Superficial incisional infection is easy to detect, but deep incisional infection is often not easily detected early. In a very small number of patients, the infection may cause life-threatening bleeding from rupture of large blood vessels in the neck.
Commonly seen after cervical lymph node dissection, it presents with a persistently high drainage volume, up to 500-1000 ml per day or more, mostly in a milky opaque fluid, also known as celiac leak. Prolonged lymphatic drainage can lead to decreased volume, electrolyte disturbance, and hypoproteinemia. When lymphatic leak occurs, drainage should be kept open. The first step is conservative treatment, usually with fasting and parenteral nutrition, and the drainage will gradually change from milky white to yellowish clear fluid in a few days, and the drainage will gradually decrease. If conservative treatment has no significant effect in 1 to 2 weeks, surgery should be considered. The surgical options are cervical thoracic duct ligation, cervical transfer tissue flap to seal the leak, or thoracoscopic ligation of the thoracic duct.
The incidence of localized effusion after thyroid surgery is approximately 1  to 6
to 6  . The greater the extent of the surgery the higher the probability of its occurrence, mainly associated with residual postoperative dead space. Retention of a drain in the operative area helps to reduce local fluid formation. Treatment includes close observation, multiple needle aspirations of the effusion, and negative pressure drainage.
. The greater the extent of the surgery the higher the probability of its occurrence, mainly associated with residual postoperative dead space. Retention of a drain in the operative area helps to reduce local fluid formation. Treatment includes close observation, multiple needle aspirations of the effusion, and negative pressure drainage.
Thyroid surgery can also cause some other complications, but the incidence is low, such as pneumothorax (caused by pleural rupture from cervical root surgery), Horner’s syndrome (injury to the sympathetic chain in the neck), tongue extension deviation due to injury to the hypoglossal nerve, and crookedness of the corners of the mouth due to injury to the mandibular rim branch of the facial nerve.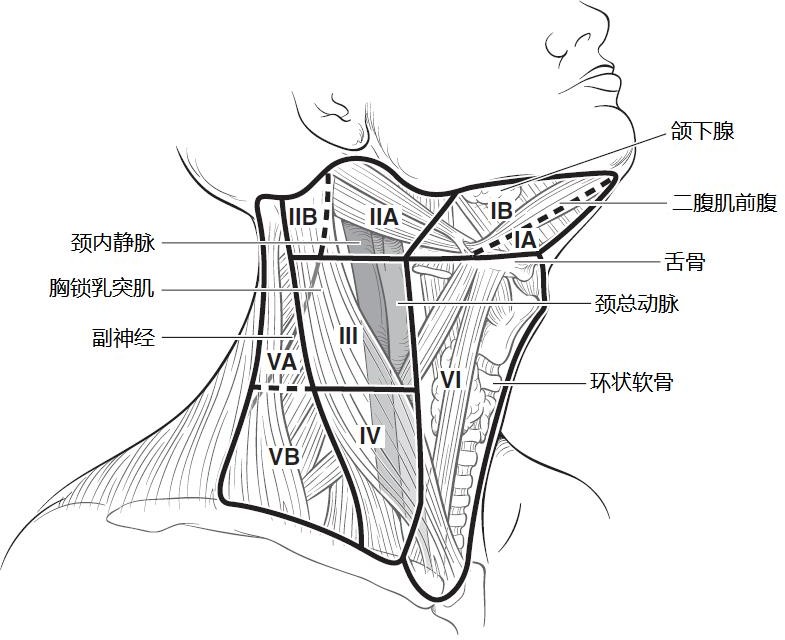
Figure 1 Cervical lymph node compartment
Table 8 Anatomic divisions of the cervical lymph node compartment
Anatomic divisions
Subdivisions
Upper border Lower border Anterior border (medial border) Posterior border (lateral border)
ⅠA Mandibular union Hyoid contralateral diastasis anterior ventral ipsilateral diastasis anterior ventral ⅠB Mandible diastasis posterior diastasis anterior ventral stem hyoid muscle
IIA
Cranial base Hyoid submarine margin flat
Stromus hyoidus Parasympathetic nerve plane
IIB Paranasal plane Posterior border of sternocleidomastoid muscle
Ⅲ Subglottis submarginal level Subcricoid level Subcricoid level Ⅳ Subcricoid level Clavicle
Sternocleidomastoid and trapezius muscles
External margin of sternocleidomastoid muscle Posterior margin of sternocleidomastoid muscle
VA
Vertex of intersection
Level of the lower edge of the cricoid cartilage
Posterior edge of sternocleidomastoid muscle Anterior edge of trapezius muscle
VB level of the inferior border of the cricoid cartilage Clavicle
VI Hyoid bone Superior border of sternal stalk Contralateral common carotid artery Ipsilateral common carotid artery
VII Superior border of sternal stalk Superior border of common carotid artery (left) Unknown artery
V. 131I therapy for differentiated thyroid cancer
Low risk of recurrence
PTC with all of the following: no distant metastases; all tumors seen visually were completely resected; tumors did not invade surrounding tissues; tumors were not an aggressive histologic subtype and did not invade blood vessels; no extra-bed iodine metastases were visualized if whole-body imaging was performed after 131I treatment; a small number of lymph node metastases were combined (e.g., cN0, but pathology revealed ≤5 micro-metastatic lymph nodes, i.e., metastases The maximum diameter of all metastases was ≤0.2 cm; follicular subtype of papillary thyroid cancer in the gland; differentiated follicular thyroid cancer in the gland with perineural invasion and with or without minor vascular invasion (<4 sites); and microscopic papillary thyroid cancer in the thyroid with or without multiple foci and with or without BRAF V600E positivity were all in the low-risk stratification.
Any 1 of the following: microscopic tumor invasion of soft tissue outside the thyroid; invasive histology (e.g., high-cell, bootstrap, columnar cell carcinoma); papillary thyroid carcinoma with vascular invasion; iodine uptake metastases in the neck on systemic imaging if treated with 131I; lymph node metastases (cN1, >5 metastatic lymph nodes on pathologic examination, all <3 cm in maximum diameter. BRAF V600E mutation-positive intraglandular papillary thyroid carcinoma (1-4 cm in diameter); BRAF V600E mutation-positive multifocal microscopic thyroid carcinoma combined with extraglandular infiltration.
- High-risk stratification
Any 1 of the following: significant extraglandular infiltration; incomplete resection of the cancer; confirmed distant metastases; high postoperative Tg levels suggestive of distant metastases; combined large lymph node metastases
(any lymph node metastasis ≧ 3 cm in diameter); extensive vascular invasion of thyroid follicular carcinoma
(>4 vascular invasion).
(b) Indications for 131I therapy.
treatment.
Patients at intermediate risk with a small number of foci or lymph node metastases, small diameter of involvement, and no risk factors such as highly invasive tissue subtypes or vascular invasion may not be treated with 131I if the overall prognosis is not improved with 131I.
- 131I therapy is not recommended for patients in the low-risk stratification.
(iii) Contraindications to 131I therapy.
(iv) 131I thyroid clearance therapy dose.
.
(v) Goals of TSH suppression therapy.
(vi) Principles of applied 131I focal clearance therapy in patients with local or distant metastases.
- 131I therapy is recommended for iodine-intake lesions that are not surgically resectable. The maximum tolerated dose is 150 mCi.
6 to 12 months. The empirical treatment dose recommendation is 100 to 200 mCi, and for patients over 70 years of age the dose is 100 to 150 mCi.
(vii) Treatment principles for Tg-positive 131I whole-body scan-negative patients.
.
VI.
External beam radiation therapy (EBRT) is only used in a small percentage of patients. In principle, radiotherapy should be used in conjunction with surgery, mainly postoperative radiotherapy.
The specific implementation should depend on the surgical resection, pathological type, lesion extent, age and other factors: (1) for less malignant cancers such as well-differentiated PTC or FTC, intervention should be considered only when re-surgical resection is not possible. ② When the tumor involves more important areas (such as tracheal wall, prevertebral tissues, larynx, arterial wall or venous aneurysm embolus) and cannot be removed surgically, and 131I therapy is ineffective or expected to be ineffective, postoperative radiation therapy can be considered. ③ For young patients, the pathological type is generally well differentiated, and they can survive with tumor for a long time even with recurrent metastasis, and both 131I treatment and reoperation are effective treatments, and the application of external radiation needs to be cautious. ④For PDTC or ATC, if there is residual or extensive lymph node metastasis after surgery, extensive postoperative radiation therapy should be given promptly to minimize the local recurrence rate and improve the prognosis.
(a) Indications for radiation therapy.
The current recommended indications for external radiation therapy are shown in Figure 2.
DTC
T4
Extensive ECE of lymph nodes
Age > 60 years
R1/2 resected
R2/not resectable
no iodine absorption
Iodine-absorbing but
Age >45 years
EBRT
IMRT recommended
Figure 2.
The indications for external radiation include: (1) those with significant residual tumors that are not surgically resectable and cannot be controlled by radionuclide therapy alone; and (2) those with postoperative residual or recurrent lesions that do not absorb iodine.
Combination therapy is the primary treatment modality and is individualized to the patient. Radiotherapy can be used as part of a combination of preoperative and postoperative treatment. Radiotherapy alone may be used, with high-dose radiotherapy (recommended dose 60Gy).
In thyroid cancer with distant metastases such as lung, liver, bone, and brain with clinical symptoms, surgery or 131I therapy combined with EBRT or stereotactic body radiation therapy can be considered to relieve symptoms and slow tumor progression.
(ii) EBRT techniques.
Detailed examination should be performed before radiotherapy to clarify the specific clearing of the tumor and to prepare for the formulation of the target area: for those who present with hoarseness, dysphagia, and wheezing indicate that the tumor has invaded the range of the thyroid body and reached the retrograde laryngeal nerve, esophagus, and trachea. Detailed examination of the neck for enlarged lymph nodes to determine whether there is regional lymph node metastasis. Laryngoscopy will be performed to determine whether there is vocal cord paralysis and whether there is invasion of the recurrent laryngeal nerve. Ultrasound and CT of the neck can be used to clarify the extent of tumor invasion and enlarged lymph nodes in the neck; CT of the lung, ultrasound of the abdomen and bone scan should be routinely examined to exclude the possibility of distant metastasis. Before postoperative radiotherapy, detailed information about surgery, postoperative residuals and postoperative pathological results should be obtained.
Conformal radiotherapy or conventional radiotherapy is available.
The best position is supine, with a properly angled head frame (to ensure maximum head extension) and headrest, and with head, neck, and shoulder thermoplastic film immobilization. The radiotherapy department of the Cancer Hospital of the Academy of Medical Sciences generally adopts C pillow, which can keep the neck in the hyperextended position.
Simulated CT scan: scan with spiral CT, all patients should be scanned with iodine contrast for enhancement, layer thickness 3mm, upper border should include the cranial vault and lower border should include all lung tissue; upload to planning system.
The design of the target area should depend on the specific circumstances, such as the type of pathology, the extent of the lesion, and the presence or absence of lymph node invasion. In general, a small field is used for highly differentiated cancers and a large field is used for poorly differentiated or undifferentiated cancers. For thyroid cancer, the upper and lower borders should be determined according to the extent of tumor invasion and the extent of lymph node metastasis, based on the principle of including the entire thyroid body and regional lymphatic drainage. For undifferentiated carcinoma, the upper border should include the upper cervical lymph nodes and the lower border should reach the level of the tracheal bifurcation to include the upper mediastinal lymph nodes.
The current treatment of the ejection field is mostly a large field treatment, which needs to include the lymph node drainage areas in the neck and upper mediastinum.
- Tumor bed (GTVtb): includes the area of preoperative tumor invasion and the extent of metastatic lymph node involvement, and should be considered as a GTVtb for outlining in cases of surgical irregularities.
The upper border of CTV2 is generally at the level of the mastoid tip and the lower border at the level of the aortic arch (if there is pathologically confirmed lymph node metastasis in the superior mediastinum, the lower border should be appropriately shifted downward).
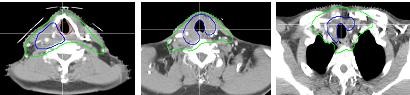
CTV1
GTVtb
p
Figure 4. Typical level of target area outline for thyroid cancer
- Prescribed dose (Figure 5):
A. Selectively treated area (or low-risk area): 50Gy-54Gy given in general. B. Highly suspicious involved area: 59.4Gy-63Gy.
C. Positive cut edge pathology area: 63Gy-66Gy. D. Sarcoplasmic residual area: 66Gy-70Gy.
E. Normal tissue limits: maximum dose of spinal cord ≤ 4000 cGy; average dose of parotid gland ≤ 2600 cGy; maximum dose of larynx ≤ 7000 cGy (no hot spots should be present in the area of larynx).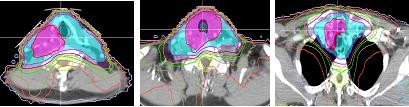

Figure 5 Typical levels of IMRT dose distribution for thyroid cancer
- Conventional radiotherapy techniques:
Figure 6 Two-front oblique field cross-angle wedge irradiation technique
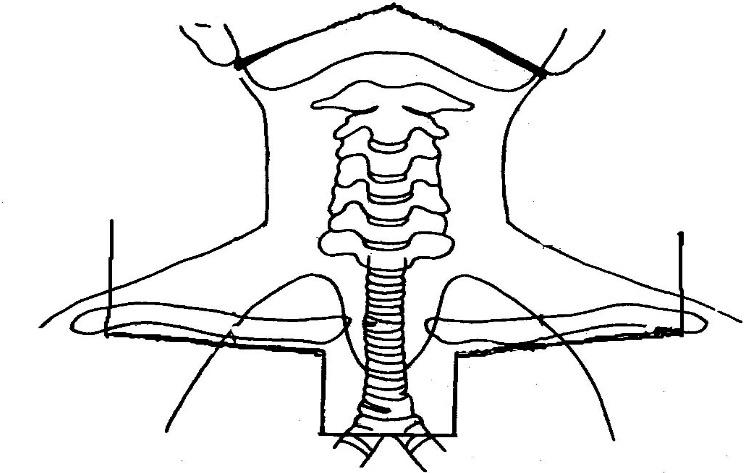 E-wire single anterior field irradiation ( However, it should be noted that this method has a large skin reaction and therefore cannot be used alone to achieve a radical dose, but can be used in combination with high-energy X-rays to achieve a radical dose.
E-wire single anterior field irradiation ( However, it should be noted that this method has a large skin reaction and therefore cannot be used alone to achieve a radical dose, but can be used in combination with high-energy X-rays to achieve a radical dose.
Figure 7 Standard fields for conventional irradiation of thyroid cancer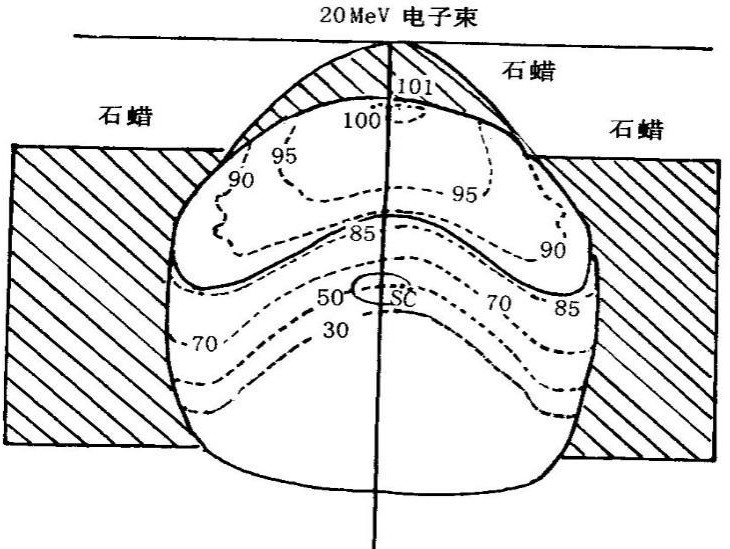
Figure 8 Dose distribution for single anterior field irradiation with 20 MeV electron beam
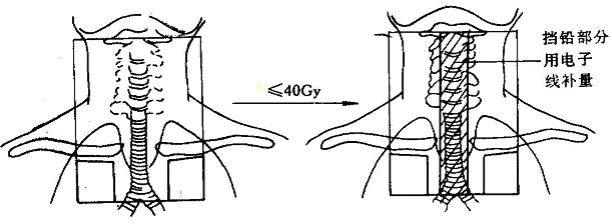 X-rays and electrons for The hybrid irradiation technique (Figure 9): first high-energy X-ray front-to-back large-field irradiation or single-anterior-field X-ray irradiation, continued X-ray irradiation with a 3-cm lead block in the anterior central neck at DT 36-40Gy, and irradiation with electrons of appropriate energy in the lead block, which ensures sufficient dose to the target area and keeps the dose to the spinal cord within the safe dose range.
X-rays and electrons for The hybrid irradiation technique (Figure 9): first high-energy X-ray front-to-back large-field irradiation or single-anterior-field X-ray irradiation, continued X-ray irradiation with a 3-cm lead block in the anterior central neck at DT 36-40Gy, and irradiation with electrons of appropriate energy in the lead block, which ensures sufficient dose to the target area and keeps the dose to the spinal cord within the safe dose range.
Figure 9 Hybrid high-energy X-ray and electron beam irradiation technique
.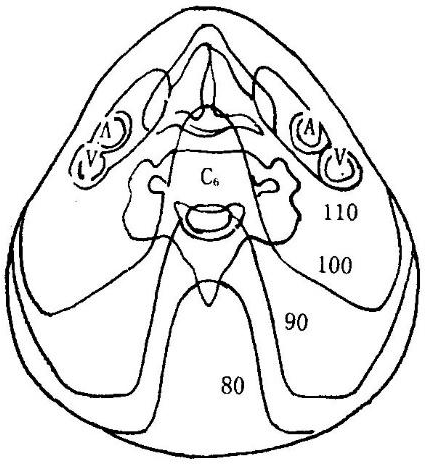
Figure 10 Dose distribution for small bucket field irradiation technique (10MV X-rays)
- Radiation source: Cobalt-60 or 4-6 MV high-energy X-rays, 8-15 MeV electron rays.
scheme) varies slightly. The conventional dose fractionation: 200 cGy in fractions, once a day, 5 times a week, 5000 cGy in the large field, followed by a reduction in the field to 6000-7000 cGy for residual areas, taking care not to exceed the tolerated spinal cord dose. Foreign treatment guidelines recommend: for lesions with
For residual lesions with visualization, 70 Gy is usually given, 66 Gy for microscopic residual or surgically removed tumors, 60 Gy for residual areas of high-risk microscopic lesions (including the thyroid bed, tracheoesophageal sulcus, and lymph node drainage area in region VI), and 54-56 Gy for low-risk microscopic lesions (including uninvaded regions III-V and upper mediastinal lymph nodes).
- EBRT complications
.
Reactions above degree 3 are rare, with the highest incidence of pharyngitis (<10  ), with the remaining reactions <5
), with the remaining reactions <5  .
.
- Distant complications: including skin-muscle fibrosis, esophageal-tracheal stenosis, pharyngeal stenosis leading to dysphagia, internal carotid artery sclerosis, and second primary cancer.
VII.
Traditional medical treatment is mainly chemotherapy, while targeted therapy and immunotherapy are new systemic treatments that have emerged in recent years. For DTC and MCT, chemotherapy is ineffective, while targeted therapy has some efficacy. The main medical treatment for ATC is chemotherapy, and targeted therapy has some efficacy.
(i) Molecular targeted therapy.
Differentiated thyroid cancer has high expression of vascular endothelial growth factor and its receptor, as well as genetic alterations such as BRAFV600E mutation, RET rearrangement, and RAS point mutation. Multikinase inhibitors acting on these targets may prolong median progression-free survival and result in tumor shrinkage in some patients.
The multikinase inhibitor sorafenib may be considered for patients with rapidly progressing, symptomatic, advanced radioiodine-refractory differentiated thyroid cancer. The approved indications for sorafenib in China are: progressive radioiodine-refractory differentiated thyroid cancer with local recurrence or metastasis.
For rapidly progressive, inoperable advanced MTC, the approved targeted therapy in China is anlotinib.
(ii) Chemotherapy.
For stage IVA and IVB ATC, chemotherapy may be considered in addition to radiation therapy. Chemotherapy can be used in tandem with radiotherapy or given adjuvantly after radiotherapy. The drugs used include paclitaxel, anthracyclines, and platinum, and the specific regimens are shown in Table 9. For concurrent chemoradiotherapy, the chemotherapy regimen is recommended as a weekly regimen.
For stage IVC undifferentiated thyroid cancer, systemic chemotherapy may be considered. Recommended regimens for stage IVC undifferentiated thyroid cancer include paclitaxel combined with platinum, doxorubicin combined with doxorubicin, paclitaxel alone, and doxorubicin alone. The specific regimens are shown in Table 10.
(iii) Immunotherapy.
Still in clinical research. For patients with thyroid cancer who have not responded to other treatments and whose disease is still progressing, participation in clinical studies related to immunotherapy is recommended.
Table 9 Adjuvant chemotherapy for stage IVA and IVB undifferentiated thyroid cancer or Table 10 Chemotherapy Regimens for Stage IVC Undifferentiated Thyroid Cancer
IV
(must be supported by polyethylene glycolated filgrastim)
Note: AUC, area under the concentration-time curve; IV, intravenous drip
VIII.
In addition, it is also closely related to deficiency, phlegm, stasis, heat, toxicity, and diet.
(II) Treatment options.
Indications: Congenital weakness or damage to the righteous qi after surgery or radiotherapy.
Representative formulas: Eight Precious Tang, Angelica Sinensis Blood Tonic Soup, Ten Perfect Tonic Soup, Tonic Zhong Yi Qi Tang plus
Decrease.
Indications: Commonly seen after radiotherapy or in vegetative deficiency. Chinese herbal tonics: Zhi Bai Di Huang Wan plus reduction
Indications: Commonly seen in bone marrow suppression or vegetative deficiency after radiotherapy. Representative tonics: Liu Wei Di Huang Wan with reduction.
Indication symptoms: depression or irritability, good tai-hui, distension and fullness and scurrying pain in the chest or less abdomen. Chinese herbal soup: Hai Zao Yu Hu Tang or Han Xia Hou Pu Tang with addition and subtraction.
6.
Indications: Superfluous masses, growing rapidly, or appearing to metastasize. Chinese herbal formula: Xihuangwan or Xiaojin Dan plus or minus.
(A) Multidisciplinary integrated treatment modalities for thyroid cancer.
Thyroid cancer, especially DTC, has a good prognosis with low mortality and long survival. It requires a multidisciplinary, standardized and integrated treatment process, including surgery, pathology, diagnostic imaging, nuclear medicine, radiotherapy, endocrinology, medical oncology, etc. Individualized and precise treatment should be implemented for different patients or different treatment stages of the same patient.
The treatment and follow-up of thyroid cancer should be led by surgery. The treatment and follow-up of thyroid cancer should be led by surgery, and a comprehensive treatment plan should be formulated in consultation with nuclear medicine, endocrinology, radiotherapy, and medical oncology according to the patient’s condition.
- For patients with low-risk differentiated thyroid cancer, surgery + postoperative exogenous thyroxine replacement therapy or TSH suppression therapy is sufficient.
/surgery + external radiotherapy. The role of surgery is primarily to relieve airway obstruction (tracheotomy) and to remove as much of the tumor as possible when conditions permit.
(b) Postoperative follow-up of thyroid cancer.
The purpose of long-term follow-up for thyroid cancer patients is to: 1. monitor those who are clinically cured for early detection of recurrent tumors and metastases; 2. dynamically observe the progress of disease and treatment effects for those who have recurrence of DTC or survive with tumors, and adjust the treatment plan; 3. monitor the effect of TSH suppression therapy; 4. To perform dynamic observation of certain concomitant diseases (e.g., heart disease, other malignancies, etc.) in DTC patients.
- Exogenous thyroxine suppression therapy is required after DTC surgery. The extent of TSH suppression therapy is determined by the risk of postoperative recurrence. After each dose adjustment of oral exogenous thyroxine, thyroid function is reviewed at 4- to 6-week follow-up intervals, which can be extended as appropriate once the desired equilibrium point is reached.
1) Patients with DTC at low to moderate risk of recurrence who have Dx-WBS that does not suggest 131I uptake outside the thyroid bed and who have no abnormal neck ultrasound and basal serum Tg levels at follow-up
(in TSH suppressed state) are not high, Dx-WBS is not required.
(ii) In patients with DTC at moderate to high risk of recurrence, the application of Dx-WBS during long-term follow-up may be valuable in detecting tumor lesions, and an examination interval of 6 to 12 months is recommended. Dx-WBS is feasible if patients have progressively higher Tg levels during follow-up or if DTC recurrence is suspected.
- CT and MRI are not routinely performed at DTC follow-up. CT or MRI of the cervical thorax should be performed if: (i) the lymph node recurrence is extensive and cannot be accurately described by ultrasound; (ii) the metastatic lesion may invade the upper aerodigestive tract and further evaluation of the extent of invasion is needed; or (iii) the serum Tg level is elevated (>10ng/ml) or TgAb is elevated in high-risk patients. If Dx-WBS is negative, iodine-containing contrast should be avoided if follow-up 131I therapy is possible. If an enhanced CT scan with iodine-contrast is performed, 131I therapy is recommended 4 to 8 weeks after the examination.
(iii) Management after detection of DTC recurrence or metastasis.
Local regional recurrence or metastasis can occur in residual thyroid tissue, soft tissues of the neck and lymph nodes, and distant metastasis can occur in the lung, bone, brain and bone marrow. The treatment options for recurrent or metastatic lesions are, in order of preference, surgical resection (for those with potential surgical cure), 131I therapy (for those with iodine uptake), external radiation therapy, observation with TSH suppression (for those with no or slow tumor progression and asymptomatic, no significant regional involvement such as the central nervous system), chemotherapy and new targeted drug therapy and approved drug clinical trials (for those with rapidly progressing disease). The final treatment regimen must take into account the patient’s needs and the patient’s needs in the clinical trials of approved drugs (refractory DTC patients with rapidly progressive disease). The final treatment plan must take into account the patient’s general status, co-morbidities and previous response to treatment. Patients with fully cleared thyroid DTC have persistently elevated serum Tg levels (>10ng/ml) at follow-up, but no lesions are detected on imaging. In this group of patients, it is possible to give
If DTC lesions or serum Tg levels are found to be reduced after treatment with Dx-WBS, 131I treatment can be repeated; otherwise, 131I treatment should be discontinued and TSH suppression therapy should be the mainstay.
(iv) Post-MTC follow-up.
Post-operative thyroid function follow-up is consistent with DTC with the exception that TSH suppressive therapy is not required. Serum calcitonin and CEA are the more specific biochemical markers for MTC and are mandatory for follow-up review. For patients whose serum calcitonin and CEA levels return to normal after surgery, the follow-up period can be referred to that of low-risk DTC; for patients whose serum calcitonin and CEA do not fall into the normal range but are at lower levels, the follow-up period can be referred to that of high-risk DTC; for patients whose biochemical parameters are still at high levels, close follow-up is recommended.
For patients with high level of biochemical indexes, close follow-up is recommended, and ultrasound should be reviewed in 3-6 months, and the extent of tumor should be confirmed according to the increase of serum calcitonin and CEA, combined with CT or MRI.
Appendix
Thyroid Cancer Guidelines (2022 Edition) Review and Validation Panel(in order of last name)
Team leader: Liu Shaoyan, Xu Zhengang
Members: Wang Ping, Wang Yu, Zhu Yiming, Sun Hui, Yang Ankui, He Xiaohui, Lin Yansong, Yi Junlin, Luo Dehong, Fang Jugao, Shi Bingyin, Qin Jianwu, Gao Ming, Guo Liang, Huang Tao, Ge Minghua, Lu Hazhen, Liao Quan
Thyroid Cancer Treatment Guidelines(2022 edition)
I. Overview
Thyroid cancer is a malignant tumor originating from the follicular epithelium or parafollicular epithelium of the thyroid gland, and is the most common malignant tumor of the head and neck. In recent years, the incidence of thyroid cancer has increased rapidly worldwide. According to the data from the National Tumor Registry, the incidence of thyroid cancer in women in urban areas in China ranks 4th among all malignant tumors in women. The incidence of
Thyroid cancer in China will continue to grow at an annual rate of 20  . The number of thyroid cancers in China will continue to grow at a rate of 20
. The number of thyroid cancers in China will continue to grow at a rate of 20  and thyroid carcinoma (TCC) based on the origin and differentiation of the tumor.<br />(Papillary Thyroid Carcinoma (PTC), Follicular Thyroid Carcinoma (FTC), Medullary Thyroid Carcinoma (MTC), Poorly Differentiated Thyroid Carcinoma (MTC), and Thyroid Carcinoma (TCC). differentiated thyroid carcinoma (PDTC) and undifferentiated thyroid cancer (ATC), of which PTC is the most common, accounting for about 90% of all thyroid cancers.<br />PTC is the most common, accounting for about 90 percent of all thyroid cancers <img decoding=) , while PTC and FTC are collectively known as Differentiated thyroid carcinoma (DTC). Different pathological types of thyroid carcinoma differ significantly in their pathogenesis, biological behavior, histological pattern, clinical presentation, treatment and prognosis. In general, DTC has a better prognosis; ATC is extremely malignant, with a median survival time of 7-10 months and a very poor prognosis; MTC has a prognosis in between.
, while PTC and FTC are collectively known as Differentiated thyroid carcinoma (DTC). Different pathological types of thyroid carcinoma differ significantly in their pathogenesis, biological behavior, histological pattern, clinical presentation, treatment and prognosis. In general, DTC has a better prognosis; ATC is extremely malignant, with a median survival time of 7-10 months and a very poor prognosis; MTC has a prognosis in between.
(a) Surveillance screening for high-risk groups.
Screening for thyroid tumors is not recommended for the general population. However, if you have a history of the following, you are at high risk for thyroid cancer and should be screened as early as possible: 1. history of childhood head and neck radiation exposure or exposure to radioactive fallout; 2. history of systemic radiation therapy; 3. history of DTC, MTC or multiple endocrine neoplasia (MEN) type II, familial polyposis, certain Prior or family history of thyroid cancer syndromes (e.g., multiple malignancy syndrome, Carney syndrome, Werner syndrome, and Gardner syndrome).
(ii) Clinical manifestations.
I. Overview
Thyroid cancer is a malignant tumor originating from the follicular epithelium or parafollicular epithelium of the thyroid gland, and is the most common malignant tumor of the head and neck. In recent years, the incidence of thyroid cancer has increased rapidly worldwide. According to the data from the National Tumor Registry, the incidence of thyroid cancer in women in urban areas in China ranks 4th among all malignant tumors in women. The incidence of
Thyroid cancer in China will continue to grow at an annual rate of 20
. The number of thyroid cancers in China will continue to grow at a rate of 20 (a) Surveillance screening for high-risk groups.
Screening for thyroid tumors is not recommended for the general population. However, if you have a history of the following, you are at high risk for thyroid cancer and should be screened as early as possible: 1. history of childhood head and neck radiation exposure or exposure to radioactive fallout; 2. history of systemic radiation therapy; 3. history of DTC, MTC or multiple endocrine neoplasia (MEN) type II, familial polyposis, certain Prior or family history of thyroid cancer syndromes (e.g., multiple malignancy syndrome, Carney syndrome, Werner syndrome, and Gardner syndrome).
(ii) Clinical manifestations.
Most patients with thyroid nodules have no clinical symptoms. They are usually detected on physical examination by palpation of the thyroid and ultrasound of the neck. Most thyroid nodules are benign, with malignant tumors accounting for about
= “wp-image-30242″ src=”https://www.kiraspecialist.com/wp-content/uploads/2022/04/1651225851-word-image.png” /> . In combination with hyper- or hypothyroidism, the corresponding clinical manifestations may occur. Benign nodules or malignant tumors of the thyroid gland can increase in size and may cause compression, often against the
It may compress the trachea and esophagus and displace the trachea and esophagus. If the malignant tumor locally encroaches on the surrounding organs, symptoms such as hoarseness, dysphagia, hemoptysis and dyspnea may also occur. MTC tumor cells secrete active substances such as calcitonin and 5-hydroxytryptamine, which can cause diarrhea, palpitations, and flushing.
The signs of thyroid cancer are mainly enlargement or nodule of thyroid gland with irregular shape, fixed adhesion to surrounding tissues, and gradually increasing in size, hard texture and unclear boundary, initially moving up and down with swallowing movement.
The nodules may initially move up and down with swallowing movements, but later they are mostly immobile. If the node is associated with cervical lymph node metastasis, the lymph nodes in the neck may be enlarged by palpation. Compression or invasion of sympathetic nerves may cause Horner syndrome.
- Invasion and metastasis
.
(The most common site of metastasis is region VI, followed by regions III, IV, II, and V. When lymph node metastasis in the lateral cervical region occurs in PTC, it is predominantly multi-regional metastasis, and only single-region metastasis is less common. Lymphatic metastases in region I are rare (<3  ). Rare lymph node metastasis sites include retropharyngeal/parapharyngeal, intraparotid, and axillary.
). Rare lymph node metastasis sites include retropharyngeal/parapharyngeal, intraparotid, and axillary.
Most thyroid cancers are differentiated thyroid cancers that grow relatively slowly, and serious complications are rare. It may cause hoarseness, dyspnea, hemoptysis, etc. due to invasion of the laryngeal nerve, trachea and other surrounding organs.
ATC is rapidly progressing and may cause severe respiratory distress.
Routine laboratory tests
The purpose is to understand the patient’s general condition and the need for appropriate therapeutic measures, including blood work, liver and kidney function, and thyroid function. If invasive testing or surgical treatment is required, coagulation and viral markers are also required. For patients with DTC who require thyroid stimulating hormone (TSH) suppression below the lower limit of the normal reference range (especially in postmenopausal women), pre-treatment baseline bone mineralization status should be evaluated and monitored regularly, depending on medical conditions; serum calcium/phosphorus, 24-hour urine calcium/phosphorus, and bone turnover biochemistry may be used.
serum calcium/phosphorus, 24-hour urinary calcium/phosphorus, and biochemical markers of bone turnover.
- Thyroid hormone, thyroid autoantibody, and tumor marker testing
)peroxidaseantibodies (TPOAb) and TSH receptor antibodies (thyrotropin receptor antibody (TRAb)). In patients with DTC, TgAb is a thyroglobulin
(thyroglobulin, Tg) is an important ancillary test. Serum Tg levels are also affected by TgAb levels, which, when present, reduce the value of the chemiluminescent immunoassay for serum Tg and affect the accuracy of monitoring the disease by Tg. The presence of TPOAb, a key enzyme in the synthesis of thyroid hormones, usually precedes thyroid dysfunction and is involved in the tissue destruction process in the development of Hashimoto’s thyroiditis and atrophic thyroiditis, causing clinical symptoms of hypothyroidism. A positive TRAb test result indicates the presence of autoantibodies against the TSH receptor.
(3) Thyroid cancer tumor marker tests: thyroglobulin (Tg)
(Tg is a specific protein produced by the thyroid gland, but serum Tg measurement lacks specific value in identifying benign and malignant thyroid nodules. Therefore, serum Tg is not used for the preoperative diagnosis of DTC, but in the post-treatment follow-up period, serum Tg is an important tool to identify whether the patient has tumor recurrence, and can be used to monitor recurrence and metastasis after DTC. For patients with DTC who have removed all thyroid tissue, elevated serum Tg indicates the possibility of tumor recurrence and should be further examined. For patients with DTC without complete thyroid removal, it is still recommended to measure serum Tg periodically (every 6 months) after surgery, and for those with persistently elevated serum Tg levels after surgery, thyroid tissue or tumor growth should be considered and further evaluation is needed in combination with other tests such as neck ultrasound.
Serum Tg measurement in DTC follow-up includes basal Tg measurement (in TSH suppressed state) and Tg measurement after TSH stimulation (TSH > 30 mU/L). To more accurately reflect the condition, serum TSH levels can be increased to >30 mU/L by discontinuing L-T4 or applying recombinant human thyrotropin (rhTSH), followed by Tg measurement after TSH stimulation, i.e., post-TSH stimulation Tg measurement. Tg levels measured after discontinuation of L-T4 and use of rhTSH were highly concordant. Patients with DTC stratified as intermediate or high risk of recurrence may be tested for post-TSH stimulation Tg if necessary. It should be noted that Tg should be tested at the same time as TgAb. If TgAb is elevated, it is not possible to determine the presence of DTC by
Tg to determine the presence or absence of recurrence of DTC. If DTC cells are poorly differentiated, unable to synthesize and secrete Tg or produce defective Tg, follow-up with Tg is also not possible. The sensitivity of detecting lymph node metastases in DTC can be improved by measuring Tg levels in lymph node puncture needle eluate for lymph nodes that are palpable on examination and for suspicious cervical lymph nodes detected by ultrasound.
Patients with MTC are recommended to have both serum calcitonin and CEA measured prior to treatment and to monitor serum levels periodically after treatment. If serum calcitonin exceeds the normal range and continues to increase, especially if calcitonin is ≥150 pg/ml, progression or recurrence should be highly suspected. Serum calcitonin and CEA tests are useful for the assessment of efficacy and monitoring of the disease in patients with myeloid carcinoma.
(4) Relevant molecular tests for diagnosis: for thyroid nodules whose benignity or malignancy cannot be determined by fine-needle aspiration (FNA), molecular markers such as BRAF mutation, RAS mutation and RET/PTC rearrangement can be tested on the puncture specimens, which can help to improve the diagnosis rate. The detection of BRAF mutations in preoperative puncture specimens can also help in the diagnosis and clinical prognosis of papillary thyroid cancer and facilitate the development of individualized diagnosis and treatment plans.
(iv) Imaging.
- Ultrasonography
This refers to an increase in nodule volume of 50  or more or at least 2 diameter lines increased by more than 20
or more or at least 2 diameter lines increased by more than 20  > (and more than 2 mm), then there is an indication for FNAB; for cystic nodules, the decision to perform FNAB should be based on the growth of the solid portion.
> (and more than 2 mm), then there is an indication for FNAB; for cystic nodules, the decision to perform FNAB should be based on the growth of the solid portion.
In postoperative thyroid patients, attention should be paid to the presence of solid lesions in the operative bed and to the presence of malignant cervical lymph nodes during follow-up. Ultrasound is difficult to identify benign lesions and recurrent lesions in the operative bed, and the evaluation of cervical lymph nodes is the same as preoperatively. The indications for postoperative puncture of suspicious cervical lymph nodes: for lymph nodes with a minimum diameter greater than 8mm and abnormal ultrasound, cytology of fine needle puncture material + eluate for Tg level can be considered; for lymph nodes smaller than 8 mm, follow-up can be performed if they do not grow or threaten the surrounding important structures.
The normal thyroid gland contains high iodine content and has a significantly different density from the surrounding tissues, which can be clearly visualized by CT plain scan, with even better contrast after contrast injection. CT scan is of great value in evaluating the extent of the thyroid tumor, its relationship with important surrounding structures such as trachea, esophagus, carotid artery and the presence of lymph node metastasis. CT has the advantage of observing the central group of lymph nodes, the upper mediastinal group of lymph nodes and the posterior pharyngeal group of lymph nodes, and can observe the posterior sternal thyroid lesions, larger lesions and their relationship with the surrounding structures, and can clearly show calcified foci of various shapes and sizes, but for nodules with a maximum diameter of ≤5 mm and However, it is not good for patients with diffuse lesions combined with nodules. For recurrent thyroid cancer, CT can provide information about the residual thyroid gland, assess the location of the lesion and its relationship with the surrounding tissues, evaluate the size and location of metastatic lymph nodes, and assess the presence of pulmonary metastases. If there is no contraindication to the use of iodine contrast.
Enhanced scans should be routinely performed for thyroid lesions. Thin layer images can reveal smaller lesions and clearly show the relationship of the lesion to surrounding tissues and organs.
The high tissue resolution allows for multi-directional and multi-parametric imaging to evaluate the extent of the lesion and its relationship to surrounding vital structures. Dynamic enhancement scans, diffusion-weighted imaging, and other functional imaging can be used to assess the benignity and malignancy of nodules. The shortcomings of MRI include insensitivity to calcification, long examination time, and susceptibility to breathing and swallowing movements.
Positron emission tomography-computed tomography (PET-CT) is not recommended as a routine test for the diagnosis of thyroid cancer, but may be considered in the following cases, if available: 1) elevated Tg (>10ng/ml) at follow-up in patients with DTC and iodine -131 (131I) diagnostic whole body scan (Dx-WBS) is negative to detect metastases.
(2) Pre-MTC staging and post-operative calcitonin elevation for metastases; (3) Pre-MTC staging and post-operative follow-up for undifferentiated thyroid cancer; (4) Pre-131I evaluation for patients with invasive or metastatic DTC (lesions showing increased PET-CT metabolism have poor iodine uptake and may not benefit from 131I therapy).
(v) Vocal fold function assessment.
Patients with thyroid cancer should be routinely evaluated for bilateral vocal fold activity preoperatively. Laryngoscopy (indirect laryngoscopy or fiberoptic laryngoscopy) can be performed. If signs of reduced or even fixed vocal fold activity are present, tumor compression or invasion of the recurrent laryngeal nerve should be highly suspected, which helps to assess the condition and surgical risk. In addition, for patients with clinical or imaging examinations (e.g., CT of the neck) suspecting tumor adjacent to or invading the trachea, preoperative fiberoptic bronchoscopy should be performed to assess whether the tumor invades the whole layer of the trachea to the tracheal lumen, as well as the extent of invasion and whether it affects the anesthetic tracheal intubation, etc., so as to formulate the corresponding surgical plan and anesthetic plan.
If tumor invasion of the recurrent laryngeal nerve is detected intraoperatively, or if intraoperative recurrent laryngeal nerve monitoring indicates that recurrent laryngeal nerve function is compromised, laryngoscopic assessment of vocal fold motor recovery is indicated postoperatively. In patients who have undergone tracheostomy or tracheotomy because of bilateral invasion of the laryngeal nerve, laryngoscopic assessment of vocal fold motion is indicated to determine the timing of removal of the tracheal tube or tracheostomy repair.
(vi) Pathology.
The cytopathologic diagnostic guidelines for thyroid cancer consist of sections on the sampling, production, and diagnostic reporting of thyroid FNA.
and a needle with an outer diameter of 5 to 5 G.FNA can be performed with a small amount of negative pressure or without negative pressure, and the needle should be performed in multiple angles and quickly. The number of needle insertions per nodule is 1 to 3, depending on the amount of needle aspiration. For cystic nodules there should be a targeted extraction of the solid zone.
- FNA production
(Table 3)
(Table 3).
Table 2 TBSRTC diagnostic grading criteria
I Non-diagnostic/unsatisfactory cyst fluid specimen
Low amount of epithelial cells
Other (e.g., blood much obscuring cells, excessive cell dryness, etc.) Ⅱ Benign
Consistent with benign follicular nodules (including adenomatous nodules and glial nodules, etc.) Consistent with Hashimoto’s thyroiditis
Consistent with subacute thyroiditis
III Atypical cells of undetermined significance/follicular lesions of undetermined significance IV Follicular neoplasm/suspected follicular neoplasm
If eosinophilic tumor, specify V Suspicious malignant
Suspected papillary thyroid carcinoma Suspected medullary thyroid carcinoma Suspected metastatic carcinoma
Suspected lymphoma VI Malignant
Papillary carcinoma of thyroid Hypofractionated carcinoma of thyroid Medullary carcinoma of thyroid Undifferentiated carcinoma of thyroid Squamous cell carcinoma
Carcinoma of mixed components (specify specific components) Metastatic malignancy
Non-Hodgkin’s lymphoma other
 Table 3 Malignant risk and clinical management for each diagnostic classification of TBSRTC
Table 3 Malignant risk and clinical management for each diagnostic classification of TBSRTC
 ~10
~10 

Follicular neoplasm/suspicious follicular



 Histopathologic Diagnostic Guidelines for Thyroid Cancer
Histopathologic Diagnostic Guidelines for Thyroid Cancer
In order to better assist clinicians in making accurate diagnosis and treatment plans, it is important to standardize thyroid histopathology so that different levels of hospitals and different pathologists can be on the same platform to communicate with each other about patient care.
.
Notes for sending frozen pathology include.
(1) Thyroid: (1) Send the specimen to the pathology department as soon as possible after isolation without any fixative.
②If the tumor nodule is <5 mm, markings (e.g., incision or tied sutures) at the tumor may be considered.
③The diagnosis of follicular thyroid tumors, including junctional tumors and follicular carcinoma, requires postoperative observation of the specimen as a whole and adequate sampling to confirm the diagnosis. (2) Lymph nodes: ①Separate the lymph nodes for examination to increase the purpose of the subdivision and the accuracy of the pathological diagnosis.
(2) Lymph nodes: ①Separate the lymph nodes for examination to increase the purpose and accuracy of pathological diagnosis. ②Send the specimens as soon as possible after isolation, keep them fresh, put them in transparent plastic pouches or specimen boxes, seal them well, and send them to the pathology department. ③The too-small specimen should not be left outside the body for too long to avoid drying and hardening, resulting in inability to freeze the film or accurate observation under the microscope. ④If sand granules are found in the lymph nodes under the pathology microscope, they should be
serial sections to look for evidence of metastasis or not. ⑤ It is not uncommon for lymph nodes to be negative for intraoperative freezing and metastatic cancer to appear in deep postoperative paraffin cuts, which needs to be informed to the patient and family as informed consent and signed before surgery or freezing.
.(vii) lymph node metastasis + extra-peritoneal invasion of lymph nodes; (viii) pTNM staging (AJCC 8th edition); (ix) immunohistochemistry as necessary.
(vii) Differential diagnosis.
III.
(A) Histologic classification of thyroid cancer.
According to the WHO definition, the histologic classification of thyroid tumors is mainly divided into primary epithelial tumors, primary non-epithelial tumors, and secondary tumors. The specific classification is shown in Table 4.
Table 4 Histologic classification of WHO thyroid tumors
Cross-sectional: Follicular tumors of undetermined malignant potential, highly differentiated tumors of undetermined malignant potential, noninvasive follicular tumors with papillary nuclei, and hyaline metachronous tumors.
Malignant: Thyroid cancer, including ① Differentiated thyroid cancer: PTC, FTC, eosinophilic carcinoma.
FTC, eosinophilic carcinoma; ②PDTC; ③ATC.
The thyroid has two different endocrine cells with different functions. About 95  of thyroid tumors arise from The rest are mostly derived from parafollicular cells of the thyroid. Mixed follicular epithelial and parafollicular cell tumors are rare, and tumor cells containing both follicular epithelial and parafollicular cell sources are of histologic origin as a
of thyroid tumors arise from The rest are mostly derived from parafollicular cells of the thyroid. Mixed follicular epithelial and parafollicular cell tumors are rare, and tumor cells containing both follicular epithelial and parafollicular cell sources are of histologic origin as a
It is controversial whether this is a separate thyroid tumor. Thyroid lymphoma is the most common tumor of non-epithelial origin of the thyroid gland and may occur independently of the thyroid gland or as part of a systemic lymphatic tumor. Thyroid sarcomas and secondary thyroid malignancies are less common in clinical practice.
PTC is the most common malignant epithelial tumor of follicular epithelial origin with characteristic PTC nuclear features. The classic PTC has two basic morphologic features: papillary and infiltrative/PTC nuclear features, with rare nuclear schwannomas and more common sandy calcifications, mainly in the lymphatic vessels or interstitium. The literature reports that 20  to 40 squamous metaplasia in 20 to 40 of cases. Lymphovascular invasion is common; vascular invasion is uncommon but can occur. Immunophenotype: TG, TTF1, PAX8, and broad-spectrum CK positive; CK20, CT, and neuroendocrine markers usually negative. The follicular subtype accounts for approximately 40 of PTC. The predominantly follicular growth pattern has the karyotype of classic PTC.
to 40 squamous metaplasia in 20 to 40 of cases. Lymphovascular invasion is common; vascular invasion is uncommon but can occur. Immunophenotype: TG, TTF1, PAX8, and broad-spectrum CK positive; CK20, CT, and neuroendocrine markers usually negative. The follicular subtype accounts for approximately 40 of PTC. The predominantly follicular growth pattern has the karyotype of classic PTC.
There are 14 subtypes of PTC, including micro PTC, encapsulated, follicular, diffuse sclerosing, sieve-mulberry, hypercellular, columnar cell, bootstrap, solid/beam, eosinophilic, worsinoma-like, clear cell, spindle cell, and papillary carcinoma with fibromatosis/fasciitis-like interstitium. The hypercellular, spike, columnar cell, and solid types are generally considered to be invasive PTCs with relatively complex genotypes and poorer prognosis than the classic types.
- Diffuse sclerosis: Most often seen in young women with diffuse bilateral or unilateral enlargement of the thyroid lobes with the serologic features of autoimmune thyroiditis. Morphologic features commonly include marked sclerosis, numerous gravelly bodies, a background of chronic lymphocytic thyroiditis, and often solid nests of tumor cells with extensive squamous metaplasia that readily invade the intrathyroidal lymph nodes
The tumor nests are often solid, with extensive squamous metaplasia, and tend to invade the intrathyroidal lymphatic ducts and extrathyroidal tissue. Molecular detection of RET rearrangements is common, while BARF mutations are rare. About 10 to 15  distant metastases occur in about 10 to 15 cases, most commonly to the lung. . Disease-free survival is shorter, but mortality is not significantly different from the common type.
distant metastases occur in about 10 to 15 cases, most commonly to the lung. . Disease-free survival is shorter, but mortality is not significantly different from the common type.
- High cell subtype: ≥30
 Cancer cells are more than 2 to 3 times as tall as they are wide, with abundant eosinophilic cytoplasm and typical PTC karyotype, often in single rows or parallel arrangements. It is more aggressive than classic type and more likely to have extrathyroidal invasion and distant metastasis. Most cases have a BRAF mutation (60
Cancer cells are more than 2 to 3 times as tall as they are wide, with abundant eosinophilic cytoplasm and typical PTC karyotype, often in single rows or parallel arrangements. It is more aggressive than classic type and more likely to have extrathyroidal invasion and distant metastasis. Most cases have a BRAF mutation (60  to 95
to 95  ).
).
.
but does not express p63, TG, TTF1, ER, β-linked proteins, and CK19.
FTC is a malignant tumor of follicular cell origin of the thyroid gland that lacks the nuclear features of papillary carcinoma, usually has an envelope, and has an infiltrative growth pattern. Incidence 6  to 10 . Subtypes include.
to 10 . Subtypes include.
(1) follicular carcinoma, microinfiltrative (envelope invasion only); (2) follicular carcinoma, intraenvelope vascular infiltration; (3) follicular carcinoma, extensive infiltration. lymph node metastasis is less common in FTC than in PTC and is more likely to occur distantly. common mutations in FTC include RAS point mutations, PAX8-PPARG fusions, TERT promoter mutations, etc. BRAF mutations and RET fusions are uncommon. BRAF mutations and RET fusions are uncommon.
Hürthle cell tumors are a group of tumors with 75 
Hürthle cell adenoma (eosinophilic adenoma) and Hürthle cell carcinoma (eosinophilic carcinoma).
3.
MTC is a malignant tumor of parafollicular cell (follicular cell) origin of the thyroid gland. Incidence 2 ~3  , sporadic and familial, with sporadic accounting for about 70% of all medullary carcinomas . The sporadic form accounts for about 70% of all medullary carcinomas
, sporadic and familial, with sporadic accounting for about 70% of all medullary carcinomas . The sporadic form accounts for about 70% of all medullary carcinomas  and is more common in the 50-60 age group. It occurs in the age group of 50-60 years, and familially at a younger age, accounting for about 30
and is more common in the 50-60 age group. It occurs in the age group of 50-60 years, and familially at a younger age, accounting for about 30 
The microscopic morphology of MTC is diverse and can resemble any thyroid malignancy, with typical structures being solid, lobulated, tubular or insular. The tumor cells are highly variable in size and can be round, polygonal, plasma cell-like, or spindle-shaped. The nuclei are low-moderate heterogeneous with relatively low nuclear fission activity.
Subtypes: There are different types based on cellular and structural features, papillary/pseudopapillary, follicular (ductal/glandular), spindle cell, giant cell, clear cell, eosinophilic, melanotic, squamous subtype, paraganglioma-like, angiosarcoma-like, small cell, and intraepithelial medullary thyroid carcinoma.
Immunohistochemical indicators: calcitonin, neuroendocrine markers (CD56, synaptophysin, chromogranin A), TTF-1, PAX8 and CEA can be expressed; TG is not expressed.
4.
PDTC are malignant tumors showing limited follicular cell differentiation and are intermediate in morphology and biological behavior between DTC and ATC. The main histological patterns are insular, beam-like and solid.
PDTC can be accompanied by varying proportions of differentiated carcinoma components, but some studies have shown that even in the presence of 10  of PDTC components are accompanied by aggressive behavior and poor prognosis. The Ki-67 index of PDTC usually ranges from 10
of PDTC components are accompanied by aggressive behavior and poor prognosis. The Ki-67 index of PDTC usually ranges from 10 
 , and the Ki-67 index in PDTC is usually between 10
, and the Ki-67 index in PDTC is usually between 10  and 30 . BCL2, CyclinD1 are usually positive, and P53, P21 and P27 are focally positive. The differential diagnosis mainly includes MTC, parathyroid carcinoma and carcinoma metastatic to the thyroid.
and 30 . BCL2, CyclinD1 are usually positive, and P53, P21 and P27 are focally positive. The differential diagnosis mainly includes MTC, parathyroid carcinoma and carcinoma metastatic to the thyroid.
ATC is a highly aggressive malignancy composed of undifferentiated thyroid follicular cells. Typical symptoms are a rapidly enlarging, hard, fixed neck mass with extensive invasion of surrounding tissues, approximately 30  to 40
to 40  Patients with distant metastases such as lung, bone and brain. The main histologic patterns are sarcomatoid, tumor giant cell-like, and epithelioid, which may occur alone or in different proportions, or may show focal squamous differentiation or heterologous differentiation; they are usually accompanied by necrosis, numerous nuclear schwannomas, and vascular invasion. Immunohistochemistry: TTF1 and TG are usually negative, PAX8 is positive in approximately half of cases, CK can be positive in areas of epithelioid differentiation, and LCA, myogenic markers, and melanoma markers are mainly used for exclusionary diagnosis. Differential diagnosis: other types of highly malignant tumors such as myogenic sarcoma, malignant melanoma, and large cell lymphoma. Highly malignant primary thyroid tumors of non-follicular and parafollicular cell origin are also generally classified as ATC, such as squamous cell carcinoma, sarcoma, mucinous epidermoid carcinoma, and others.
Patients with distant metastases such as lung, bone and brain. The main histologic patterns are sarcomatoid, tumor giant cell-like, and epithelioid, which may occur alone or in different proportions, or may show focal squamous differentiation or heterologous differentiation; they are usually accompanied by necrosis, numerous nuclear schwannomas, and vascular invasion. Immunohistochemistry: TTF1 and TG are usually negative, PAX8 is positive in approximately half of cases, CK can be positive in areas of epithelioid differentiation, and LCA, myogenic markers, and melanoma markers are mainly used for exclusionary diagnosis. Differential diagnosis: other types of highly malignant tumors such as myogenic sarcoma, malignant melanoma, and large cell lymphoma. Highly malignant primary thyroid tumors of non-follicular and parafollicular cell origin are also generally classified as ATC, such as squamous cell carcinoma, sarcoma, mucinous epidermoid carcinoma, and others.
(b) Staging of thyroid cancer.
Clinical staging can be established based on preoperative assessment (history, physical examination, ancillary tests)
(cTNM). Pathologic staging (pTNM) was obtained based on postoperative pathologic findings. The specific staging criteria are shown in Tables 5 and 6 (AJCC 8th edition).
Table 5 Definition of TNM staging
carcinoma
organs and soft tissues such as larynx, trachea, esophagus, laryngeal denervation and subcutaneous soft tissues
artery, mediastinal vessels
or upper mediastinum) lymph nodes, either unilaterally or bilaterally
III, IV, or V areas) or retropharyngeal lymph node metastases
Table 6 TNM staging of thyroid cancer
Period
Period
Period
Period
Period
Period
Period
stage
Period
Period
Period
Period
stage
Period
A number of characteristics of the tumor will affect the prognosis of the tumor. Some of the more important factors include tissue type, primary tumor size, extraglandular invasion, vascular infiltration, BRAF mutations, and distant metastases.
- Tissue type: Survival rates for patients with PTC are generally good, but tumor mortality varies widely between specific subtypes. Among these, the hypercellular, shoe-peg, columnar cell, and solid types are the aggressive subtypes.
FTC is typically characterized by isolated tumors with an envelope and is more aggressive than PTC. fTC usually has microfollicular structures and is diagnosed as carcinoma because of infiltration of follicular cells into the envelope or blood vessels. the prognosis is worse for those with infiltration into blood vessels than for those with infiltration into the envelope. Highly invasive FTCs are uncommon and are often seen to invade surrounding tissues and blood vessels intraoperatively. Approximately 80 of highly invasive FTCs will distant metastases, which can lead to approximately 20  of patients die within a few years of diagnosis. Poor prognosis is strongly associated with older age, higher tumor stage, and larger tumor size at the time of diagnosis.
of patients die within a few years of diagnosis. Poor prognosis is strongly associated with older age, higher tumor stage, and larger tumor size at the time of diagnosis.
PTC has a similar prognosis to FTC, with both having a better prognosis if the tumor is confined to the thyroid, is less than 1 cm in diameter, or is minimally metastatic. If distant metastases and high invasiveness are present, the prognosis is poor.
- Primary tumor size: Papillary carcinoma <1 cm, called microscopic carcinoma, is usually found on physical examination and has an almost zero lethality rate and a low risk of recurrence. However, microscopic cancer is not always a tumor with a low risk of recurrence. For example, about 20
 of multifocal microscopic cancers There is also a risk of distant metastasis.
of multifocal microscopic cancers There is also a risk of distant metastasis.
The size of the primary tumor is associated with prognosis and mortality. It has been shown that DTC with primary tumors <1.5 cm in maximum diameter are less likely to develop distant metastases, while larger tumors (>1.5 cm) have a recurrence rate of approximately 33% within 30 years  . The 30-year mortality rate of DTC with a maximum diameter <1.5cm is 0.4
. The 30-year mortality rate of DTC with a maximum diameter <1.5cm is 0.4  and 7 for larger tumors (>1.5 cm)
and 7 for larger tumors (>1.5 cm)  .
.
- Local invasion: approximately 10
 of DTC invade surrounding organs/structures, and the local recurrence rate is approximately twice that of non-invasive tumors. Patients with invasive cancer also have elevated mortality, with approximately 1 in 3 patients dying.
of DTC invade surrounding organs/structures, and the local recurrence rate is approximately twice that of non-invasive tumors. Patients with invasive cancer also have elevated mortality, with approximately 1 in 3 patients dying.
cancer and in patients >40 years of age (35 
The overall prognosis of DTC is good, with relatively low mortality. However, disease recurrence rates vary widely depending on clinicopathologic features. Patients were classified into 3 strata of risk of recurrence based on intraoperative pathologic features such as residual lesions, tumor size and number, pathologic subtypes, envelope vascular invasion, lymph node metastasis and extravasation, postoperative Tg levels after TSH stimulation (sTg), and molecular pathologic features (Table 7). Postoperative adjuvant therapy is strongly recommended for DTC in the high-risk group; adjuvant therapy can be considered in the intermediate-risk group; 131I thyroid clearance is generally not indicated in the low-risk group, but endocrine therapy should be considered.
Table 7 Clinicopathologic features of DTC recurrence risk stratification
No residual tumor without extranodal invasion of the bulk of the tumor
Non-malignant histologic subtype
No iodine uptake foci outside the thyroid bed without vascular invasion on first post-operative whole-body nuclide scan
cN0 or less than 5 small lymph node metastases (<0.2 cm in diameter)
Follicular subtype PTC, located within the thyroid, not breaching the envelope; tiny thyroid papillae
FTC, located in the thyroid gland, well differentiated, with envelope invasion and no vascular invasion, or only minimal vascular invasion
Microinvasion of peri-thyroidal tissue
first postoperative nuclear imaging with iodine uptake in the neck lesion
Highly malignant subtype (hypercellular, columnar cell, diffuse sclerosis, etc.) with vascular invasion
cN1 or pN1 with more than 5 lymph node metastases and metastases less than 3 cm in diameter
Multifocal papillary microcarcinoma of the thyroid with or without BRAF V600E mutation
Obvious invasion of soft tissue tumor remnants around the thyroid
Distant metastasis
High postoperative serum Tg suggesting distant metastasis
pN1 and metastatic lymph node metastases ≥3 cm in diameter
Extensive vascular invasion of follicular thyroid cancer (>4 vascular invasions)
IV.
(a) Surgical treatment of thyroid cancer.
Treatment of DTC is primarily surgical, supplemented by postoperative endocrine therapy, radionuclide therapy, and in some cases, radiation therapy and targeted therapy. mtc is primarily surgical, supplemented in some cases by radiation therapy and targeted therapy. In the treatment of undifferentiated cancer, a few patients have the opportunity to undergo surgery, and some patients may have some effect with radiotherapy and chemotherapy, but the overall prognosis is very poor and survival time is short. However, the overall prognosis is very poor and survival time is short. It should also be noted that individualization of tumor treatment is very important, and each patient’s condition and demands are different, so there is some flexibility in clinical diagnosis and treatment.
A subset of T1 lesions are low-risk micro papillary carcinomas. Because of its relatively slow progression and low lethality, conservative therapy, which involves active surveillance and close follow-up, can be considered in addition to surgical treatment. Low-risk papillary carcinoma that can be closely monitored generally has the following characteristics: (1) the primary tumor is a single lesion, (2) the maximum diameter of the primary lesion is <1 cm, (3) the location of the primary lesion is located in the central part of the thyroid gland rather than immediately adjacent to the thyroid peritoneum or trachea, and (4) there are no regional lymph node metastases after evaluation. In addition to the above conditions, the patient should be considered for any history of high dose radiation exposure during early childhood, thyroid cancer, and the presence of a metastatic node.
In addition to the above, specific factors such as history of exposure to high doses of ionizing radiation during childhood, family history of thyroid cancer, and the presence of hyperthyroidism should be considered. If closely monitored, re-evaluation is usually required every 6 months. If the evaluation reveals progression of the primary tumor (e.g., 2-3 mm in diameter, new tumor lesions, or clinically suspicious metastatic regional lymph nodes), discontinuation of conservative treatment should be considered.
For T3 lesions with large tumors or those that have invaded the extraperitoneal muscles of the thyroid, total thyroidectomy is recommended. However, for lesions closer to the thyroid peritoneum, which may not be large per se but have invaded the extraperitoneal muscles, excision of the affected lobe and isthmus, together with excision of the invaded muscles, may be performed. The specific surgical options are recommended, weighing the benefits and risks of surgery.
For T4 lesions that have invaded the surrounding structures, total thyroidectomy is usually recommended; for T4a lesions, removal of the thyroid gland along with partial removal of the affected structures, such as part of the larynx (or even the whole larynx), part of the airways, and the larynx.
(T4b lesions are generally considered to be inoperable, but the possibility of surgery is determined on a case-by-case basis and may require multidisciplinary collaboration with vascular surgery, orthopedics, and neurosurgery. In general, however, T4b lesions are difficult to completely resect, have a poor prognosis, are associated with higher surgical risks, and have more postoperative complications. Surgical treatment requires careful evaluation of the condition, with a focus on whether the patient will benefit from surgery. Sometimes, palliative decompression therapy is necessary, such as a tracheotomy to relieve dyspnea.
- Management of regional lymph nodes: central zone lymph nodes (zone VI): cN1a The affected central zone should be cleared. If the lesion is on one side, it is recommended that the central zone be cleared to include the affected tracheoesophageal groove and the anterior trachea. The anterior laryngeal region is also part of the central zone sweep, but the anterior laryngeal gonad
The metastasis to the nodes is rare and can be individualized. For patients with cN0, central zone clearance may be considered in the presence of high-risk factors (e.g., T3 to T4 lesions, multifocal carcinoma, family history, history of early childhood ionizing radiation exposure). For low-risk patients with cN0 (without high-risk factors), the treatment can be individualized. The extent of central zone clearance is defined as the level of the superior border of the innominate artery at the inferior border, the level of the hyoid bone at the superior border, and the medial border of the common carotid artery at the lateral border, including the anterior trachea. The right tracheoesophageal groove requires attention to the lymphatic adipose tissue at the deep level where the laryngeal recurrent nerve is located. Central
If the parathyroid glands cannot be preserved in situ, parathyroid autotransplantation should be performed.
Lateral cervical lymph node dissection (zones I-V): Lateral cervical lymph node metastases are most often seen in zones III and IV, followed by zones II and V. Zone I is less common. Lateral cervical lymph node dissection is recommended for therapeutic dissection, i.e., lateral cervical dissection when N1b is confirmed by preoperative evaluation or intraoperative freezing. The recommended scope of lateral neck dissection includes zones II, III, IV, and VB, with zones IIA, III, and IV being the smallest. Zone I does not require routine clearance. The schematic diagram of the neck partition and the specific division of each zone are shown in Figure 1 and Table 8.
The parapharyngeal lymph nodes, upper mediastinal lymph nodes, and other special areas of lymph nodes are recommended for simultaneous surgical resection when metastasis is considered on imaging.
For MTC, total thyroidectomy is recommended. In the case of MTC diagnosed after lobectomy, a total thyroidectomy is recommended. In individual cases, sporadic microscopic MTC found incidentally after lobectomy may also be considered for close observation.
MTC is more prone to cervical lymph node metastases, and most patients have lymph node metastases at the time of presentation, so removal of the primary site should be accompanied by cervical lymph node dissection (central or lateral cervical area), the extent of which should be determined by serum calcitonin levels in addition to clinical evaluation.
Some MTCs are hereditary myeloid carcinomas and can be treated by detecting germline mutations in the RET gene.
(The diagnosis can be made by testing for germline mutations in the RET gene (by genetic testing of somatic cells or blood leukocytes). In this group, total thyroidectomy and cervical lymph node dissection are recommended. In the case of MEN II patients, the systemic situation should be evaluated. Pheochromocytoma, for example, needs to be managed before considering thyroid surgery.
A small number of patients with undifferentiated cancer have small tumors at the time of presentation and may have access to surgery. Most patients with undifferentiated cancer have a large and rapidly progressing neck mass at the time of presentation and have no chance of surgery. Tracheotomy can be considered when the tumor compresses the trachea and causes respiratory distress.
In addition to conventional rehydration, dexamethasone and neurotrophic drugs can be given as adjunctive therapy to reduce neuroedema after thyroid cancer surgery. In patients with total thyroidectomy, parathyroid hormone and blood calcium should be reviewed, and those with low calcium should be given calcium supplements and oral vitamin D and calcium as soon as they can eat. Patients with injury to one laryngeal nerve often choke on food and water during the acute phase. If necessary, a tracheotomy kit should be placed at the bedside. Patients with bilateral laryngeal return nerve injury are usually treated intraoperatively with a tracheal tube and postoperative care of the tracheotomy opening. For patients with cervical lymph node dissection, postoperative attention should be paid to the functional exercise of the neck and shoulder.
Postoperative care should be paid to the functional exercise of the neck and shoulder. A postoperative adjuvant treatment plan should be developed and communicated to the patient according to pathologic staging and risk stratification.
(b) Common postoperative complications.
Surgical complications are other surgically related conditions that occur during the surgical treatment of disease and have a certain probability of occurring and are not completely avoidable.
The incidence of bleeding after thyroid cancer surgery is about 1  to 2
to 2  or so, most often within within 24 hours after surgery. The main manifestations are increased, bloody drainage, swelling of the neck, and difficulty in breathing. If the drainage is >100 ml/h, active bleeding is considered and prompt debridement should be performed to stop the bleeding. If the patient is in respiratory distress, the airway should be controlled first, and the bedside incision can be opened in an emergency to relieve the pressure of the hematoma on the trachea first. Risk factors for postoperative bleeding in thyroid cancer include combined hypertension, anticoagulant medications, or aspirin.
or so, most often within within 24 hours after surgery. The main manifestations are increased, bloody drainage, swelling of the neck, and difficulty in breathing. If the drainage is >100 ml/h, active bleeding is considered and prompt debridement should be performed to stop the bleeding. If the patient is in respiratory distress, the airway should be controlled first, and the bedside incision can be opened in an emergency to relieve the pressure of the hematoma on the trachea first. Risk factors for postoperative bleeding in thyroid cancer include combined hypertension, anticoagulant medications, or aspirin.
The incidence probability of laryngeal nerve injury in thyroid surgery is reported in the literature as 0.3  ~15.4
~15.4  . Common causes of injury to the recurrent laryngeal nerve include tumor adhesion or invasion of the nerve, and the cause of surgical operation. If the tumor invades the laryngeal nerve, the tumor can be removed or the nerve can be removed together, depending on the situation. If the nerve is resected, it is recommended to perform one-stage nerve grafting or repair if possible. Injury to the laryngeal nerve on one side, postoperative paralysis of the vocal cords on the same side, hoarseness and choking on water. The surgical operation itself may damage the recurrent laryngeal nerve, and this condition cannot be completely avoided. Bilateral laryngeal nerve injury, postoperative respiratory distress can occur, life-threatening, surgery should be performed at the same time tracheotomy to ensure the airway is open.
. Common causes of injury to the recurrent laryngeal nerve include tumor adhesion or invasion of the nerve, and the cause of surgical operation. If the tumor invades the laryngeal nerve, the tumor can be removed or the nerve can be removed together, depending on the situation. If the nerve is resected, it is recommended to perform one-stage nerve grafting or repair if possible. Injury to the laryngeal nerve on one side, postoperative paralysis of the vocal cords on the same side, hoarseness and choking on water. The surgical operation itself may damage the recurrent laryngeal nerve, and this condition cannot be completely avoided. Bilateral laryngeal nerve injury, postoperative respiratory distress can occur, life-threatening, surgery should be performed at the same time tracheotomy to ensure the airway is open.
Injury to the superior laryngeal nerve, the patient’s voice becomes muffled after surgery. Intraoperative management of the supraglottic artery should be performed with close dissection of the thyroid gland to reduce the probability of supraglottic nerve injury.
The intraoperative neuromonitoring (IONM) technique can help to localize the recurrent laryngeal nerve intraoperatively, to detect the function of the recurrent laryngeal nerve after the specimen is lowered, and to locate the injured segment if there is nerve damage. IONM is recommended for secondary surgery, large thyroid masses, and preoperative nerve palsy on one side, when available.
Fine dissection along the peritoneum, intraoperative exposure of the recurrent laryngeal nerve, proper use of energy instruments, and standard use of IONM can reduce the probability of nerve injury.
The incidence of postoperative permanent is about 2  ~15
~15  , mostly after total thyroid This is usually seen after total thyroid removal. The main manifestation is postoperative hypocalcemia, with patients experiencing tingling of the hands and feet, perioral numbness, or twitching of the hands and feet, which is relieved by intravenous calcium drips. For temporary hypoparathyroidism, calcium can be given to relieve the symptoms, with the addition of osteopontin if necessary. Prophylactic dosing may be considered to reduce postoperative symptoms. In permanent hypoparathyroidism, lifelong calcium and vitamin D supplements are required. Intraoperative attention should be paid to the fine dissection along the perineurium and to the protection of the blood supply when the parathyroid glands are preserved in situ. Some staining techniques can assist in the intraoperative identification of the parathyroid glands, such as nano-carbon negative contrast.
, mostly after total thyroid This is usually seen after total thyroid removal. The main manifestation is postoperative hypocalcemia, with patients experiencing tingling of the hands and feet, perioral numbness, or twitching of the hands and feet, which is relieved by intravenous calcium drips. For temporary hypoparathyroidism, calcium can be given to relieve the symptoms, with the addition of osteopontin if necessary. Prophylactic dosing may be considered to reduce postoperative symptoms. In permanent hypoparathyroidism, lifelong calcium and vitamin D supplements are required. Intraoperative attention should be paid to the fine dissection along the perineurium and to the protection of the blood supply when the parathyroid glands are preserved in situ. Some staining techniques can assist in the intraoperative identification of the parathyroid glands, such as nano-carbon negative contrast.
Thyroid surgery is mostly a type I incision, with a small number of type II incisions involving the larynx, trachea, and esophagus. The incidence of postoperative thyroid incision infection is approximately 1  to 2
to 2  . The risk of incisional infection
. The risk of incisional infection
Factors include cancer, diabetes, and immunocompromise. The signs of incisional infection include fever, cloudy drainage, redness and oozing of the incision, increased skin temperature, and local pain with pressure. If incisional infection is suspected, antibiotic treatment should be given promptly, and the incision should be opened and changed if there is abscess accumulation. Superficial incisional infection is easy to detect, but deep incisional infection is often not easily detected early. In a very small number of patients, the infection may cause life-threatening bleeding from rupture of large blood vessels in the neck.
Commonly seen after cervical lymph node dissection, it presents with a persistently high drainage volume, up to 500-1000 ml per day or more, mostly in a milky opaque fluid, also known as celiac leak. Prolonged lymphatic drainage can lead to decreased volume, electrolyte disturbance, and hypoproteinemia. When lymphatic leak occurs, drainage should be kept open. The first step is conservative treatment, usually with fasting and parenteral nutrition, and the drainage will gradually change from milky white to yellowish clear fluid in a few days, and the drainage will gradually decrease. If conservative treatment has no significant effect in 1 to 2 weeks, surgery should be considered. The surgical options are cervical thoracic duct ligation, cervical transfer tissue flap to seal the leak, or thoracoscopic ligation of the thoracic duct.
The incidence of local effusion after thyroid surgery is approximately 1  to 6 . The greater the extent of surgery the higher the probability of its occurrence, mainly associated with residual postoperative dead space. Retention of a drain in the operative area helps to reduce local fluid formation. Treatment includes close observation, multiple needle aspirations of the effusion, and negative pressure drainage.
to 6 . The greater the extent of surgery the higher the probability of its occurrence, mainly associated with residual postoperative dead space. Retention of a drain in the operative area helps to reduce local fluid formation. Treatment includes close observation, multiple needle aspirations of the effusion, and negative pressure drainage.
Thyroid surgery can also cause some other complications, but the incidence is low, such as pneumothorax (caused by pleural rupture from cervical root surgery), Horner’s syndrome (injury to the sympathetic chain in the neck), tongue extension deviation due to injury to the hypoglossal nerve, and crookedness of the corners of the mouth due to injury to the mandibular rim branch of the facial nerve.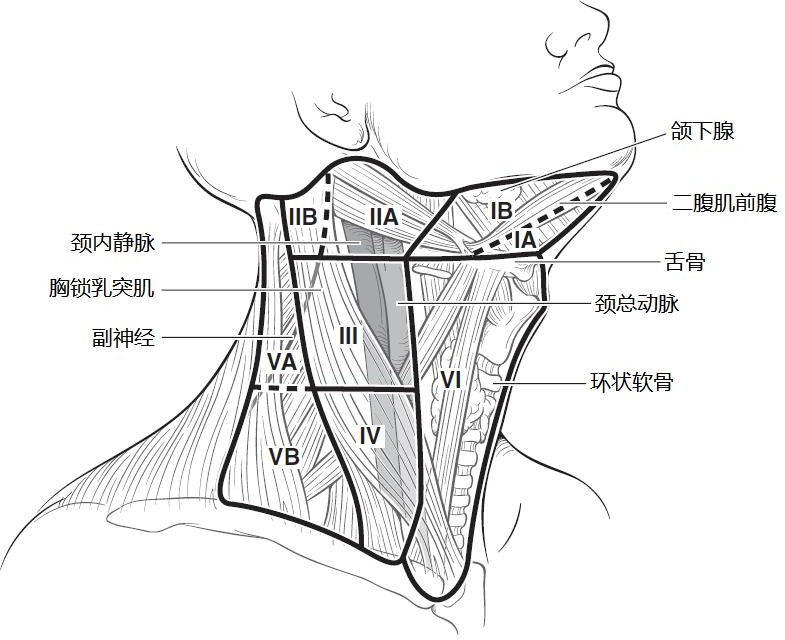
Figure 1 Cervical lymph node compartment
Table 8 Anatomic divisions of the cervical lymph node compartment
Anatomic divisions
Subdivisions
Upper border Lower border Anterior border (medial border) Posterior border (lateral border)
ⅠA Mandibular union Hyoid contralateral diastasis anterior ventral ipsilateral diastasis anterior ventral ⅠB Mandible diastasis posterior diastasis anterior ventral stem hyoid muscle
IIA
Cranial base Hyoid submarine margin flat
Stromus hyoidus Parasympathetic nerve plane
IIB Paranasal plane Posterior border of sternocleidomastoid muscle
Ⅲ Subglottis submarginal level Subcricoid level Subcricoid level Ⅳ Subcricoid level Clavicle
Sternocleidomastoid and trapezius muscles
External margin of sternocleidomastoid muscle Posterior margin of sternocleidomastoid muscle
VA
Vertex of intersection
Level of the lower edge of the cricoid cartilage
Posterior edge of sternocleidomastoid muscle Anterior edge of trapezius muscle
VB level of the inferior border of the cricoid cartilage Clavicle
VI Hyoid bone Superior border of sternal stalk Contralateral common carotid artery Ipsilateral common carotid artery
VII Superior border of sternal stalk Superior border of common carotid artery (left) Unknown artery
V. 131I therapy for differentiated thyroid cancer
Low risk of recurrence
PTC with all of the following: no distant metastases; all tumors seen visually were completely resected; tumors did not invade surrounding tissues; tumors were not an aggressive histologic subtype and did not invade blood vessels; no extra-bed iodine metastases were visualized if whole-body imaging was performed after 131I treatment; a small number of lymph node metastases were combined (e.g., cN0, but pathology revealed ≤5 micro-metastatic lymph nodes, i.e., metastases The maximum diameter of all metastases was ≤0.2 cm; follicular subtype of papillary thyroid cancer in the gland; differentiated follicular thyroid cancer in the gland with perineural invasion and with or without minor vascular invasion (<4 sites); and microscopic papillary thyroid cancer in the thyroid with or without multiple foci and with or without BRAF V600E positivity were all in the low-risk stratification.
Any 1 of the following: microscopic tumor invasion of soft tissue outside the thyroid; invasive histology (e.g., high-cell, bootstrap, columnar cell carcinoma); papillary thyroid carcinoma with vascular invasion; iodine uptake metastases in the neck on systemic imaging if treated with 131I; lymph node metastases (cN1, >5 metastatic lymph nodes on pathologic examination, all <3 cm in maximum diameter. BRAF V600E mutation-positive intraglandular papillary thyroid carcinoma (1-4 cm in diameter); BRAF V600E mutation-positive multifocal microscopic thyroid carcinoma combined with extraglandular infiltration.
- High-risk stratification
Any 1 of the following: significant extraglandular infiltration; incomplete resection of the cancer; confirmed distant metastases; high postoperative Tg levels suggestive of distant metastases; combined large lymph node metastases
(any lymph node metastasis ≧ 3 cm in diameter); extensive vascular invasion of thyroid follicular carcinoma
(>4 vascular invasion).
(b) Indications for 131I therapy.
treatment.
Patients at intermediate risk with a small number of foci or lymph node metastases, small diameter of involvement, and no risk factors such as highly invasive tissue subtypes or vascular invasion may not be treated with 131I if the overall prognosis is not improved with 131I.
- 131I therapy is not recommended for patients in the low-risk stratification.
(iii) Contraindications to 131I therapy.
(iv) 131I thyroid clearance therapy dose.
.
(v) Goals of TSH suppression therapy.
(vi) Principles of applied 131I focal clearance therapy in patients with local or distant metastases.
- 131I therapy is recommended for iodine-intake lesions that are not surgically resectable. The maximum tolerated dose is 150 mCi.
6 to 12 months. The empirical treatment dose recommendation is 100 to 200 mCi, and for patients over 70 years of age the dose is 100 to 150 mCi.
(vii) Treatment principles for Tg-positive 131I whole-body scan-negative patients.
.
VI.
External beam radiation therapy (EBRT) is only used in a small percentage of patients. In principle, radiotherapy should be used in conjunction with surgery, mainly postoperative radiotherapy.
The specific implementation should depend on the surgical resection, pathological type, lesion extent, age and other factors: (1) for less malignant cancers such as well-differentiated PTC or FTC, intervention should be considered only when re-surgical resection is not possible. ② When the tumor involves more important areas (such as tracheal wall, prevertebral tissues, larynx, arterial wall or venous aneurysm embolus) and cannot be removed surgically, and 131I therapy is ineffective or expected to be ineffective, postoperative radiation therapy can be considered. ③ For young patients, the pathological type is generally well differentiated, and they can survive with tumor for a long time even with recurrent metastasis, and both 131I treatment and reoperation are effective treatments, and the application of external radiation needs to be cautious. ④For PDTC or ATC, if there is residual or extensive lymph node metastasis after surgery, extensive postoperative radiation therapy should be given promptly to minimize the local recurrence rate and improve the prognosis.
(a) Indications for radiation therapy.
The current recommended indications for external radiation therapy are shown in Figure 2.
DTC
T4
Extensive ECE of lymph nodes
Age > 60 years
R1/2 resected
R2/not resectable
no iodine absorption
Iodine-absorbing but
Age >45 years
EBRT
IMRT recommended
Figure 2.
The indications for external radiation include: (1) those with significant residual tumors that are not surgically resectable and cannot be controlled by radionuclide therapy alone; and (2) those with postoperative residual or recurrent lesions that do not absorb iodine.
Combination therapy is the primary treatment modality and is individualized to the patient. Radiotherapy can be used as part of a combination of preoperative and postoperative treatment. Radiotherapy alone may be used, with high-dose radiotherapy (recommended dose 60Gy).
In thyroid cancer with distant metastases such as lung, liver, bone, and brain with clinical symptoms, surgery or 131I therapy combined with EBRT or stereotactic body radiation therapy can be considered to relieve symptoms and slow tumor progression.
(ii) EBRT techniques.
Detailed examination should be performed before radiotherapy to clarify the specific clearing of the tumor and to prepare for the formulation of the target area: for those who present with hoarseness, dysphagia, and wheezing indicate that the tumor has invaded the range of the thyroid body and reached the retrograde laryngeal nerve, esophagus, and trachea. Detailed examination of the neck for enlarged lymph nodes to determine whether there is regional lymph node metastasis. Laryngoscopy will be performed to determine whether there is vocal cord paralysis and whether there is invasion of the recurrent laryngeal nerve. Ultrasound and CT of the neck can be used to clarify the extent of tumor invasion and enlarged lymph nodes in the neck; CT of the lung, ultrasound of the abdomen and bone scan should be routinely examined to exclude the possibility of distant metastasis. Before postoperative radiotherapy, detailed information about surgery, postoperative residuals and postoperative pathological results should be obtained.
Conformal radiotherapy or conventional radiotherapy is available.
The best position is supine, with a properly angled head frame (to ensure maximum head extension) and headrest, and with head, neck, and shoulder thermoplastic film immobilization. The radiotherapy department of the Cancer Hospital of the Academy of Medical Sciences generally adopts C pillow, which can keep the neck in the hyperextended position.
Simulated CT scan: scan with spiral CT, all patients should be scanned with iodine contrast for enhancement, layer thickness 3mm, upper border should include the cranial vault and lower border should include all lung tissue; upload to planning system.
The design of the target area should depend on the specific circumstances, such as the type of pathology, the extent of the lesion, and the presence or absence of lymph node invasion. In general, a small field is used for highly differentiated cancers and a large field is used for poorly differentiated or undifferentiated cancers. For thyroid cancer, the upper and lower borders should be determined according to the extent of tumor invasion and the extent of lymph node metastasis, based on the principle of including the entire thyroid body and regional lymphatic drainage. For undifferentiated carcinoma, the upper border should include the upper cervical lymph nodes and the lower border should reach the level of the tracheal bifurcation to include the upper mediastinal lymph nodes.
The current treatment of the ejection field is mostly a large field treatment, which needs to include the lymph node drainage areas in the neck and upper mediastinum.
- Tumor bed (GTVtb): includes the area of preoperative tumor invasion and the extent of metastatic lymph node involvement, and should be considered as a GTVtb for outlining in cases of surgical irregularities.
The upper border of CTV2 is generally at the level of the mastoid tip and the lower border at the level of the aortic arch (if there is pathologically confirmed lymph node metastasis in the superior mediastinum, the lower border should be appropriately shifted downward).
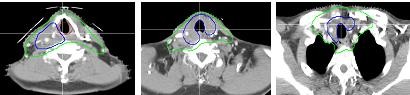
CTV1
GTVtb
p
Figure 4. Typical level of target area outline for thyroid cancer
- Prescribed dose (Figure 5):
A. Selectively treated area (or low-risk area): 50Gy-54Gy given in general. B. Highly suspicious involved area: 59.4Gy-63Gy.
C. Positive cut edge pathology area: 63Gy-66Gy. D. Sarcoplasmic residual area: 66Gy-70Gy.
E. Normal tissue limits: maximum dose of spinal cord ≤ 4000 cGy; average dose of parotid gland ≤ 2600 cGy; maximum dose of larynx ≤ 7000 cGy (no hot spots should be present in the area of larynx).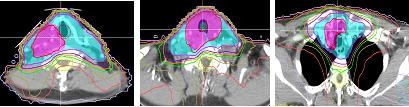

Figure 5 Typical levels of IMRT dose distribution for thyroid cancer
- Conventional radiotherapy techniques:
Figure 6 Two-front oblique field cross-angle wedge irradiation technique
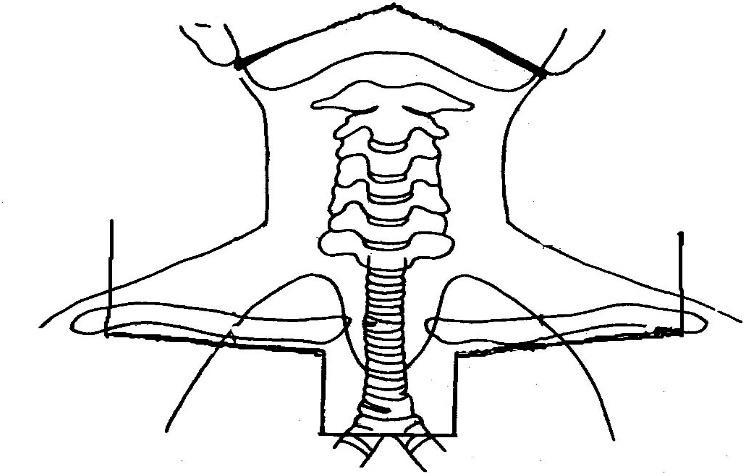 E-wire single anterior field irradiation ( However, it should be noted that this method has a high skin response and therefore cannot be used alone to achieve a radical dose, but can be used in combination with high-energy X-rays to achieve a radical dose.
E-wire single anterior field irradiation ( However, it should be noted that this method has a high skin response and therefore cannot be used alone to achieve a radical dose, but can be used in combination with high-energy X-rays to achieve a radical dose.
Figure 7 Standard fields for conventional irradiation of thyroid cancer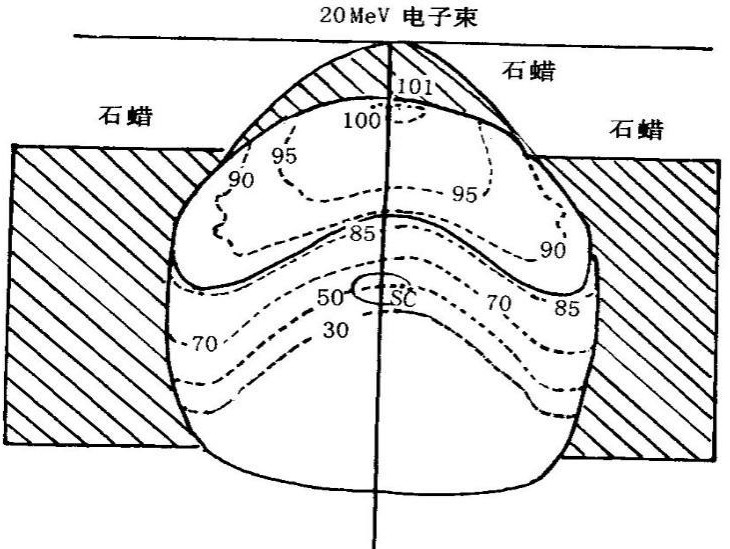
Figure 8 Dose distribution for single anterior field irradiation with 20 MeV electron beam
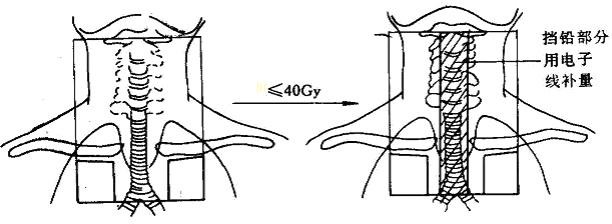 X-rays and electrons for The hybrid irradiation technique (Figure 9): first high-energy X-ray front-to-back large-field irradiation or single anterior field X-ray irradiation, 3 cm of lead blocking in the center of the anterior neck at DT 36-40Gy to continue the X-ray irradiation, and the lead blocking part is irradiated with electrons of appropriate energy, which ensures sufficient dose to the target area and keeps the exposure to the spinal cord within the safe dose range.
X-rays and electrons for The hybrid irradiation technique (Figure 9): first high-energy X-ray front-to-back large-field irradiation or single anterior field X-ray irradiation, 3 cm of lead blocking in the center of the anterior neck at DT 36-40Gy to continue the X-ray irradiation, and the lead blocking part is irradiated with electrons of appropriate energy, which ensures sufficient dose to the target area and keeps the exposure to the spinal cord within the safe dose range.
Figure 9 Hybrid high-energy X-ray and electron beam irradiation technique
.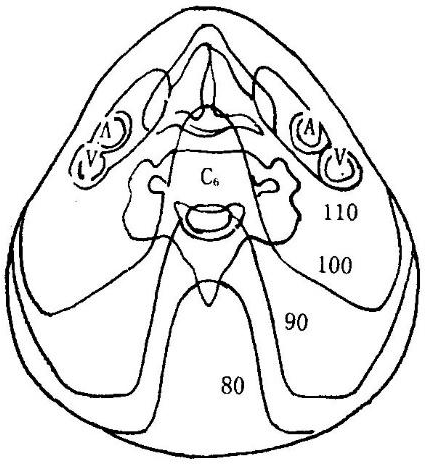
Figure 10 Dose distribution for small bucket field irradiation technique (10MV X-rays)
- Radiation source: Cobalt-60 or 4-6 MV high-energy X-rays, 8-15 MeV electron rays.
scheme) varies slightly. The conventional dose fractionation: 200 cGy in fractions, once a day, 5 times a week, 5000 cGy in the large field, followed by a reduction in the field to 6000-7000 cGy for residual areas, taking care not to exceed the tolerated spinal cord dose. Foreign treatment guidelines recommend: for lesions with
For residual lesions with visualization, 70 Gy is usually given, 66 Gy for microscopic residual or surgically removed tumors, 60 Gy for residual areas of high-risk microscopic lesions (including the thyroid bed, tracheoesophageal sulcus, and lymph node drainage area in region VI), and 54-56 Gy for low-risk microscopic lesions (including uninvaded regions III-V and upper mediastinal lymph nodes).
- EBRT complications
.
Reactions above degree 3 are rare, with the highest incidence of pharyngitis (<10  ), with the remaining reactions being <5
), with the remaining reactions being <5  .
.
- Distant complications: including skin-muscle fibrosis, esophageal-tracheal stenosis, pharyngeal stenosis leading to dysphagia, internal carotid artery sclerosis, and second primary cancer.
VII.
Traditional medical treatment is mainly chemotherapy, while targeted therapy and immunotherapy are new systemic treatments that have emerged in recent years. For DTC and MCT, chemotherapy is ineffective, while targeted therapy has some efficacy. The main medical treatment for ATC is chemotherapy, and targeted therapy has some efficacy.
(i) Molecular targeted therapy.
Differentiated thyroid cancer has high expression of vascular endothelial growth factor and its receptor, as well as genetic alterations such as BRAFV600E mutation, RET rearrangement, and RAS point mutation. Multikinase inhibitors acting on these targets may prolong median progression-free survival and result in tumor shrinkage in some patients.
The multikinase inhibitor sorafenib may be considered for patients with rapidly progressing, symptomatic, advanced radioiodine-refractory differentiated thyroid cancer. The approved indications for sorafenib in China are: progressive radioiodine-refractory differentiated thyroid cancer with local recurrence or metastasis.
For rapidly progressive, inoperable advanced MTC, the approved targeted therapy in China is anlotinib.
(ii) Chemotherapy.
For stage IVA and IVB ATC, chemotherapy may be considered in addition to radiation therapy. Chemotherapy can be used in tandem with radiotherapy or given adjuvantly after radiotherapy. The drugs used include paclitaxel, anthracyclines, and platinum, and the specific regimens are shown in Table 9. For concurrent chemoradiotherapy, the chemotherapy regimen is recommended as a weekly regimen.
For stage IVC undifferentiated thyroid cancer, systemic chemotherapy may be considered. Recommended regimens for stage IVC undifferentiated thyroid cancer include paclitaxel combined with platinum, doxorubicin combined with doxorubicin, paclitaxel alone, and doxorubicin alone. The specific regimens are shown in Table 10.
(iii) Immunotherapy.
Still in clinical research. For patients with thyroid cancer who have not responded to other treatments and whose disease is still progressing, participation in clinical studies related to immunotherapy is recommended.
Table 9 Adjuvant chemotherapy for stage IVA and IVB undifferentiated thyroid cancer or Table 10 Chemotherapy Regimens for Stage IVC Undifferentiated Thyroid Cancer
IV
(must be supported by polyethylene glycolated filgrastim)
Note: AUC, area under the concentration-time curve; IV, intravenous drip
VIII.
In addition, it is also closely related to deficiency, phlegm, stasis, heat, toxicity, and diet.
(II) Treatment options.
Indications: Congenital weakness or damage to the righteous qi after surgery or radiotherapy.
Representative formulas: Eight Precious Tang, Angelica Sinensis Blood Tonic Soup, Ten Perfect Tonic Soup, Tonic Zhong Yi Qi Tang plus
Decrease.
Indications: Commonly seen after radiotherapy or in vegetative deficiency. Chinese herbal tonics: Zhi Bai Di Huang Wan plus reduction
Indications: Commonly seen in bone marrow suppression or vegetative deficiency after radiotherapy. Representative tonics: Liu Wei Di Huang Wan with reduction.
Indication symptoms: depression or irritability, good tai-hui, distension and fullness and scurrying pain in the chest or less abdomen. Chinese herbal soup: Hai Zao Yu Hu Tang or Han Xia Hou Pu Tang with addition and subtraction.
6.
Indications: Superfluous masses, growing rapidly, or appearing to metastasize. Chinese herbal formula: Xihuangwan or Xiaojin Dan plus or minus.
(A) Multidisciplinary integrated treatment modalities for thyroid cancer.
Thyroid cancer, especially DTC, has a good prognosis with low mortality and long survival. It requires a multidisciplinary, standardized and integrated treatment process, including surgery, pathology, diagnostic imaging, nuclear medicine, radiotherapy, endocrinology, medical oncology, etc. Individualized and precise treatment should be implemented for different patients or different treatment stages of the same patient.
The treatment and follow-up of thyroid cancer should be led by surgery. The treatment and follow-up of thyroid cancer should be led by surgery, and a comprehensive treatment plan should be formulated in consultation with nuclear medicine, endocrinology, radiotherapy, and medical oncology according to the patient’s condition.
- For patients with low-risk differentiated thyroid cancer, surgery + postoperative exogenous thyroxine replacement therapy or TSH suppression therapy is sufficient.
/surgery + external radiotherapy. The role of surgery is primarily to relieve airway obstruction (tracheotomy) and to remove as much of the tumor as possible when conditions permit.
(b) Postoperative follow-up of thyroid cancer.
The purpose of long-term follow-up for thyroid cancer patients is to: 1. monitor those who are clinically cured for early detection of recurrent tumors and metastases; 2. dynamically observe the progress of disease and treatment effects for those who have recurrence of DTC or survive with tumors, and adjust the treatment plan; 3. monitor the effect of TSH suppression therapy; 4. To perform dynamic observation of certain concomitant diseases (e.g., heart disease, other malignancies, etc.) in DTC patients.
- Exogenous thyroxine suppression therapy is required after DTC surgery. The extent of TSH suppression therapy is determined by the risk of postoperative recurrence. After each dose adjustment of oral exogenous thyroxine, thyroid function is reviewed at 4- to 6-week follow-up intervals, which can be extended as appropriate once the desired equilibrium point is reached.
1) Patients with DTC at low to moderate risk of recurrence who have Dx-WBS that does not suggest 131I uptake outside the thyroid bed and who have no abnormal neck ultrasound and basal serum Tg levels at follow-up
(in TSH suppressed state) are not high, Dx-WBS is not required.
(ii) In patients with DTC at moderate to high risk of recurrence, the application of Dx-WBS during long-term follow-up may be valuable in detecting tumor lesions, and an examination interval of 6 to 12 months is recommended. Dx-WBS is feasible if patients have progressively higher Tg levels during follow-up or if DTC recurrence is suspected.
- CT and MRI are not routinely performed at DTC follow-up. CT or MRI of the cervical thorax should be performed if: (i) the lymph node recurrence is extensive and cannot be accurately described by ultrasound; (ii) the metastatic lesion may invade the upper aerodigestive tract and further evaluation of the extent of invasion is needed; or (iii) the serum Tg level is elevated (>10ng/ml) or TgAb is elevated in high-risk patients. If Dx-WBS is negative, iodine-containing contrast should be avoided if follow-up 131I therapy is possible. If an enhanced CT scan with iodine-contrast is performed, 131I therapy is recommended 4 to 8 weeks after the examination.
(iii) Management after detection of DTC recurrence or metastasis.
Local regional recurrence or metastasis can occur in residual thyroid tissue, soft tissues of the neck and lymph nodes, and distant metastasis can occur in the lung, bone, brain and bone marrow. The treatment options for recurrent or metastatic lesions are, in order of preference, surgical resection (for those with potential surgical cure), 131I therapy (for those with iodine uptake), external radiation therapy, observation with TSH suppression (for those with no or slow tumor progression and asymptomatic, no significant regional involvement such as the central nervous system), chemotherapy and new targeted drug therapy and approved drug clinical trials (for those with rapidly progressing disease). The final treatment regimen must take into account the patient’s needs and the patient’s needs in the clinical trials of approved drugs (refractory DTC patients with rapidly progressive disease). The final treatment plan must take into account the patient’s general status, co-morbidities and previous response to treatment. Patients with fully cleared thyroid DTC have persistently elevated serum Tg levels (>10ng/ml) at follow-up, but no lesions are detected on imaging. In this group of patients, it is possible to give
If DTC lesions or serum Tg levels are found to be reduced after treatment with Dx-WBS, 131I treatment can be repeated; otherwise, 131I treatment should be discontinued and TSH suppression therapy should be the mainstay.
(iv) Post-MTC follow-up.
Post-operative thyroid function follow-up is consistent with DTC with the exception that TSH suppressive therapy is not required. Serum calcitonin and CEA are the more specific biochemical markers for MTC and are mandatory for follow-up review. For patients whose serum calcitonin and CEA levels return to normal after surgery, the follow-up period can be referred to that of low-risk DTC; for patients whose serum calcitonin and CEA do not fall into the normal range but are at lower levels, the follow-up period can be referred to that of high-risk DTC; for patients whose biochemical parameters are still at high levels, close follow-up is recommended.
For patients with high level of biochemical indexes, close follow-up is recommended, and ultrasound should be reviewed in 3-6 months, and the extent of tumor should be confirmed according to the increase of serum calcitonin and CEA, combined with CT or MRI.
Appendix