Review plan
The review plan is different for patients with different stages of esophageal cancer. Patients with stage I-III esophagus are usually treated with radical aim such as surgery. The risk of recurrence is highest within 2 to 3 years after the end of treatment. Therefore, patients with stage I to III esophageal cancer should undergo imaging every 6 months for 2 to 3 years after treatment for surveillance follow-up in order to detect recurrence in a timely manner. After 2 years of treatment, patients should undergo annual imaging surveillance to detect abnormalities.
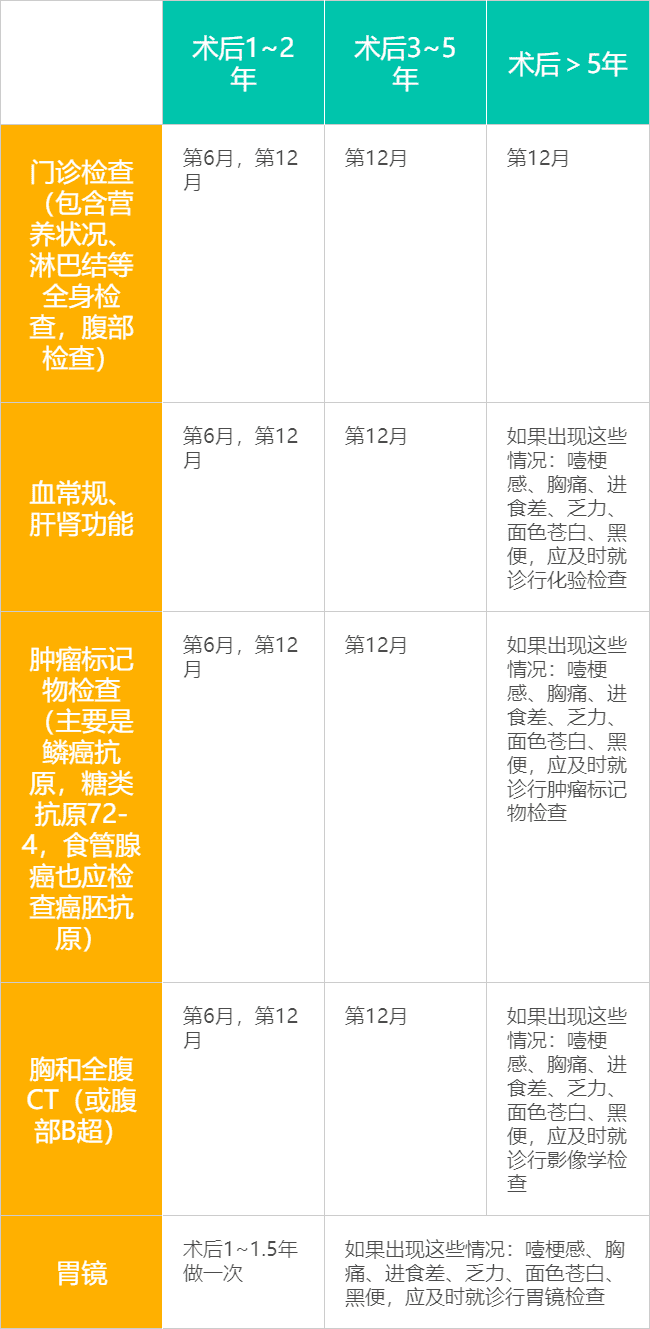
Follow-up schedule for patients with stage I esophageal cancer
Follow-up schedule for patients with stage II esophageal cancer
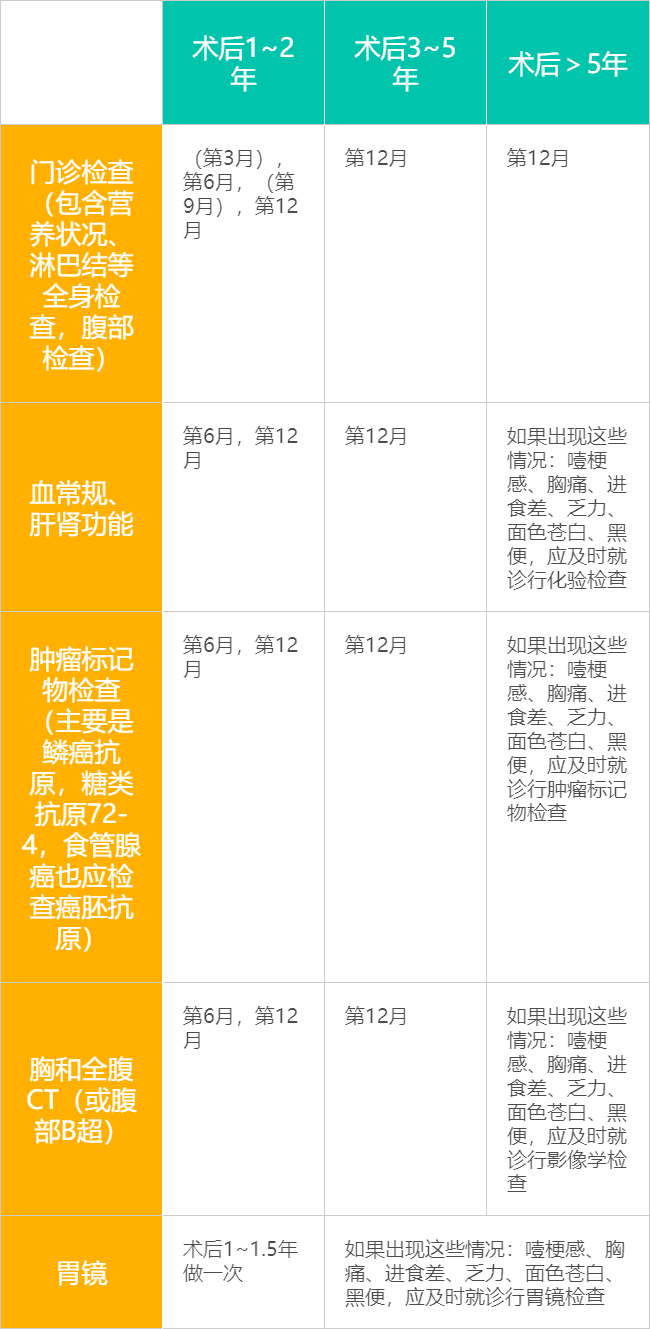
Note: Parentheses are optional depending on the patient’s situation, especially for patients with high risk factors for recurrence and patients with precancerous lesions such as Barrett’s esophagus, who may be reviewed more frequently as appropriate due to elevated risk of recurrence.
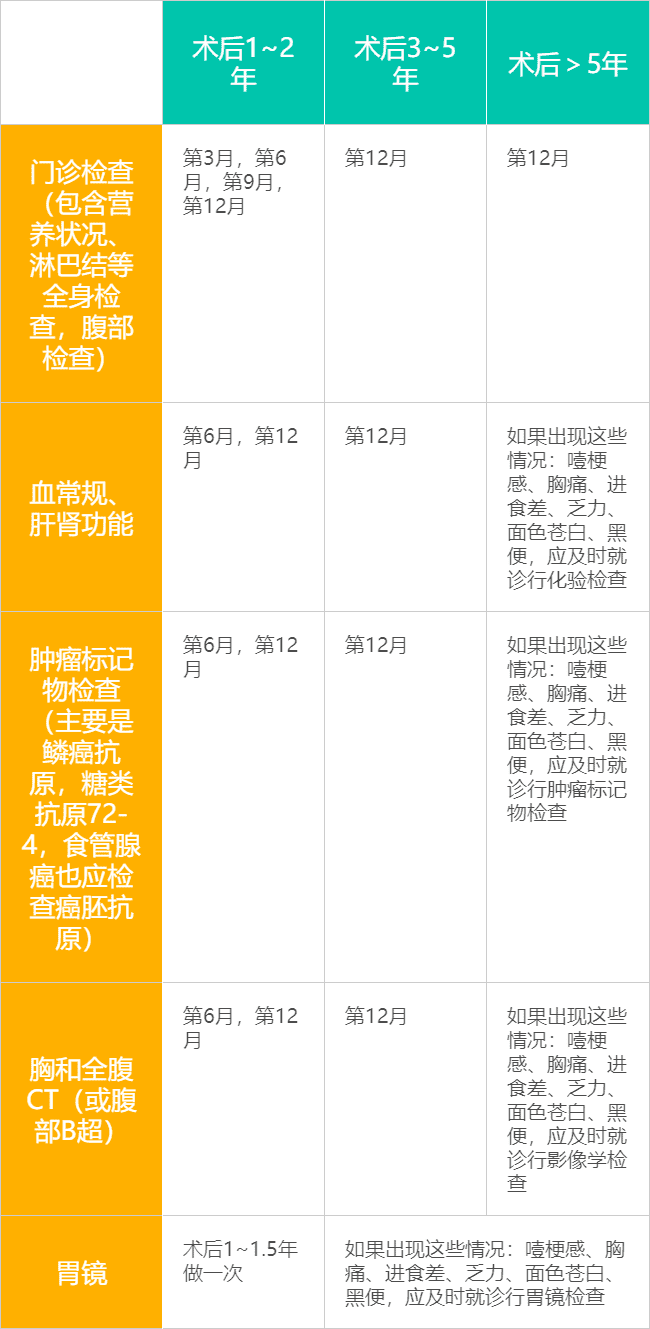
Follow-up schedule for patients with stage III esophageal cancer
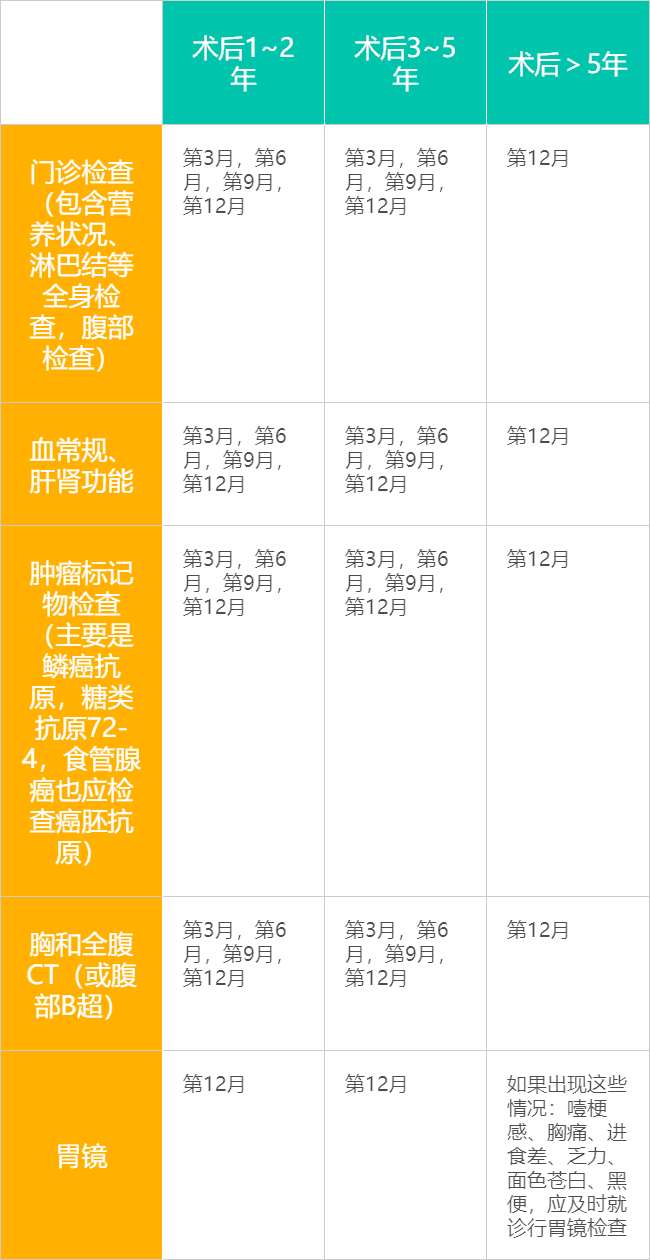
Stage IV esophageal cancer is incurable, and patients usually undergo chemotherapy, immunotherapy, or targeted therapy focused on prolonging survival and relieving symptoms. Because of the high risk of progression in advanced esophageal cancer, systemic examinations and imaging assessments should be performed every 3 months after the end of treatment to detect tumor progression early.
Follow-up schedule for patients with stage IV esophageal cancer
Cautions
- Reviews should be performed as prescribed by the physician, at the time and in accordance with the items prescribed by the physician.
- At each review, bring the initial imaging and pathology reports, along with imaging films of all initial and most recent lesions (chest and whole abdomen CT films), and medical records such as treatment course notes.
- Describe clearly the recent symptoms, especially new discomfort such as choking sensation, dysphagia, chest pain, epigastric pain, poor feeding, black stool, weakness, pallor, and weight loss.
- Any psychological problems should also be promptly described to the physician.
- Keep a record, such as noting the time of the next review, precautions to take, and symptoms that the doctor cautions need extra attention. If you need to take medication, record in detail how to take it, the duration of treatment, adverse reactions and monitoring indicators.
.
Indicators requiring special attention
General
Esophageal cancer patients need to have their weight measured regularly, and they need to promptly report to their physicians if they experience significant weight loss or weakness or fever in a short period of time without obvious reasons.
Laboratory tests
Some patients with esophageal cancer may suffer from malnutrition and anemia due to the disease and treatment, and chemotherapy may also cause anemia, leukopenia, and impairment of liver and kidney function, etc. After treatment is completed, blood tests and liver and kidney function should also be reviewed regularly to understand treatment complications and recovery of organ function.
- Blood tests, alert for bone marrow suppression
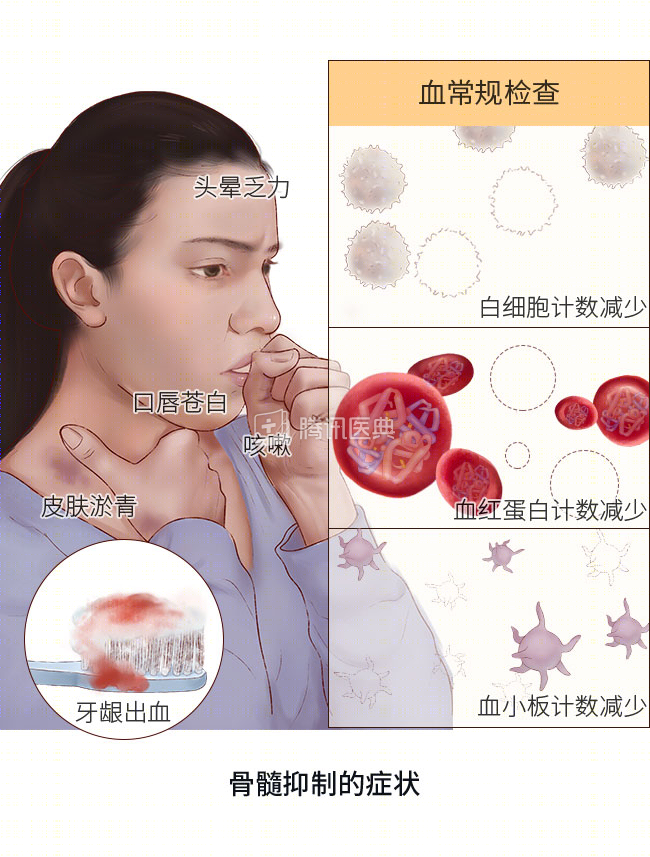
If the report shows white blood cells <3.0×109/L, hemoglobin <90 g/L, and platelets <75×109/L, there is a possibility of bone marrow suppression or other abnormalities.
Myelosuppression is a common adverse effect of chemotherapy in patients with esophageal cancer, and patients often experience varying degrees of hemoglobin, white blood cell, or platelet reduction. Physical manifestations include dizziness and weakness; pale lips and mouth; susceptibility to infection (e.g., easy to catch a cold, fever, or cough); tendency to cause skin bruising; and bleeding symptoms such as bleeding gums. Bone marrow suppression not only delays chemotherapy and thus affects the effectiveness of treatment, but may also lead to life-threatening complications. Therefore, once the possibility of bone marrow suppression is detected, the doctor needs to be contacted for treatment at the first opportunity.
- Blood tests, beware of anemia and malnutrition following you
Because some patients have difficulty eating after esophageal cancer surgery, many patients with esophageal cancer will develop anemia and malnutrition. Therefore, it is necessary to test indicators reflecting nutritional status, such as vitamin B12, folic acid, and iron, in patients who do not eat well, especially if they have a combination of pallor, weakness, palpitations, and lethargy. If the report shows nutritional deficiencies and severe deficiencies in hematopoietic raw materials, the physician should be informed promptly and timely supplementation should be provided through meals, supplements and oral nutrition solutions.
- Liver and kidney function tests to prevent liver and kidney impairment
Any abnormal elevation of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin, as well as a blood creatinine higher than the upper limit of normal, on the liver and kidney function test report should alert you to the presence of treatment-related liver and kidney impairment and require prompt consultation with your doctor for further testing.
- Tumor marker values to watch
Esophageal cancer patients need to be tested for tumor-related markers for esophageal cancer. Patients with squamous carcinoma should be concerned about indicators such as squamous carcinoma antigen and glycoconjugate antigen 72-4, and patients with esophageal adenocarcinoma should also be concerned about carcinoembryonic antigen, which is correlated with tumor disease and may indicate tumor recurrence when elevated. It is worth noting, however, that sometimes infection, inflammation, drugs and other factors can also cause tumor markers to rise, so once there is a sudden and rapid rise in indicators, you should promptly inform your doctor and promptly perform imaging examinations to exclude recurrence and metastasis.
Imaging
Esophageal cancer patients should have regular review of chest CT and whole abdomen CT for timely detection of tumor recurrence and metastases to organs such as the liver. If the report suggests abnormalities such as esophageal swelling, enlargement of the original lesion or new lesions, you should promptly ask your doctor to review the films to clarify the nature of the lesions and to determine whether the tumor has recurred and metastasized.
Gastroscopy
The role of gastroscopy in the post-treatment review of patients with esophageal cancer is controversial. It is generally accepted that review should be noted at the initial diagnosis or 1 to 1.5 years after surgery to detect tumor recurrence in a timely manner, especially in patients with high risk factors for recurrence such as late staging or precancerous lesions such as Barrett’s esophagus, which should be reviewed at the onset of clinical symptoms.