Endoscopic resection is a minimally invasive treatment that requires the use of an endoscopic electric knife to remove the lesion. Therefore, endoscopic surgery is not 100% safe.
But in general, the incidence of all types of complications with endoscopic resection therapy is relatively low. The commonly used endoscopic submucosal dissection (ESD), for example, has a perforation rate of 0% to 6%, an almost 0% postoperative bleeding rate, and a local recurrence rate of 0.9% to 1.2%.
There are 3 main categories of risks associated with endoscopic resection: bleeding, perforation, and stenosis.
Hemorrhage
It is well understood that anything that is operated on is bound to bleed.
Endoscopic resection is along the submucosa to peel away the lesions in the mucosal layer. The submucosa has a rich vascular network, and during resection, the electric knife may damage the blood vessels in the submucosa, causing bleeding.
Small bleeds are common and can usually be safely stopped endoscopically. However, if a large arterial bleed occurs, endoscopy cannot safely stop the bleeding, and emergency surgical open-heart surgery is then required to stop the bleeding. However, the probability of major arterial bleeding is very low and is prevented by the surgeon during surgery, so you do not need to worry too much.
Perforation
Surgical resection too deep, leading to perforation
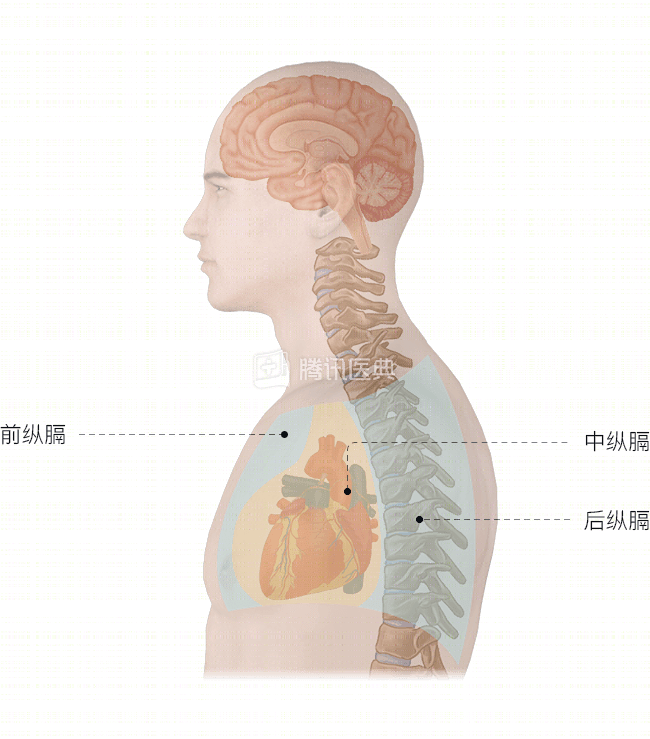
The esophageal wall is only a few millimeters thick, and if the endoscopic resection is too deep, it can cut through the esophageal wall and lead to perforation. This also means that the esophageal lumen and the mediastinum are penetrated. The mediastinum is sterile, while the esophageal lumen is lined with bacteria. The perforation may cause mucus or gas from the esophageal lumen to enter the mediastinum and cause infection.
Small perforations can usually be sutured through endoscopy, and the risk of mediastinal infection is low.
Larger perforations, which cannot be closed by the surgeon through endoscopic suturing, require urgent open-heart surgical management. However, the probability of this occurring in an experienced hospital is extremely low, and you do not need to worry too much.
Late perforation
After endoscopic surgery, it is usually not necessary to suture the surgical wound. The wound heals well on its own in about 1 to 2 months after surgery. During the healing process, because the endoscopically removed esophageal area is relatively thin (equivalent to a watermelon with its rind cut off) and the esophagus itself secretes some mucus, eating after surgery can be irritating to the trauma. Within 7 days after surgery, there is a risk of perforation due to irritation of the trabeculae, also known as delayed perforation.
Although the incidence of delayed perforation is low, when it occurs, the patient develops a mediastinal infection that requires surgical debridement and drainage.
Stenosis
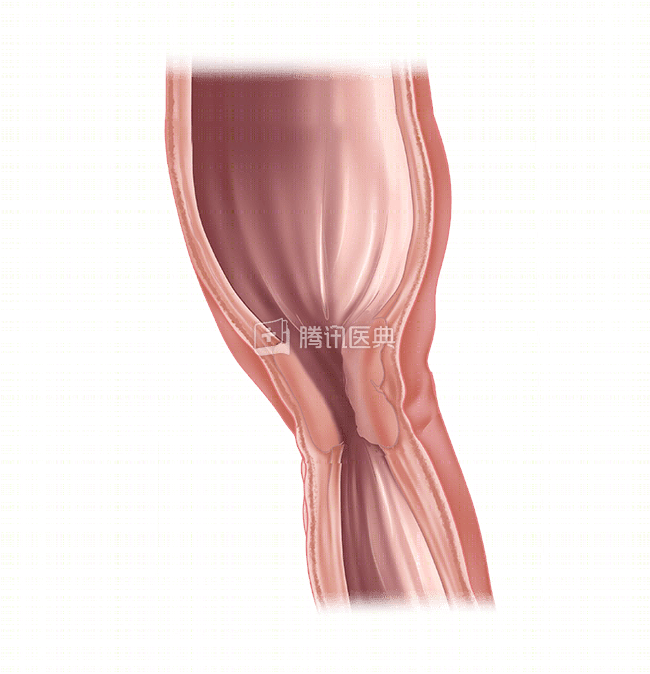
The esophageal lumen is a cylindrical cavity. If the endoscopic resection area exceeds 3/4 of a week of the lumen, or if the resection site is close to the esophageal inlet or lower cardia, luminal stricture is likely to occur. In severe cases, this can result in the patient being unable to eat (Figure).
After surgery, the surgeon will use a number of options to prevent and treat the narrowing of the esophageal lumen, including probe or balloon dilation, temporary stent placement, and drug prophylaxis.
In addition to the 3 major complications above, chest pain and painful swallowing are also more common after treatment. To prevent them, it is recommended that you do not eat hard and hotter foods after surgery to avoid irritating the mucosa and worsening the pain. If the pain is severe, you can take oral pain medication to relieve it under the guidance of your doctor. If your temperature exceeds 38.5°C, or if your symptoms do not resolve or even get worse, please contact your primary care physician promptly.