With advances in surgical techniques, the rate of surgical death and postoperative complications of hepatocellular carcinoma has decreased dramatically, and surgical resection of hepatocellular carcinoma is recognized as the safe and effective first choice for hepatocellular carcinoma treatment. However, the high postoperative recurrence rate remains a major factor affecting patients’ long-term survival.
Most recurrences arise from primary tumors through microvascular invasion and peripheral spread, which are considered to be the most important factors associated with poor prognosis. In this regard, the surgical community has been exploring more effective resection methods.
Proposal of anatomic hepatic segmental resection
Systematic hepatic resection is thought to be more effective in eradicating intrahepatic metastases from hepatocellular carcinoma. Systematic hepatectomy, which is the removal of a segment of the liver associated with a portal vein, is also known as anatomic resection (AR).
In contrast, most surgeons prefer to leave a larger portion of thin-walled tissue in this functional unit, such as nonanatomic resection (NAR), which focuses on preserving ≥1 cm of tumor-free margins to reduce postoperative liver failure and cirrhosis in patients.
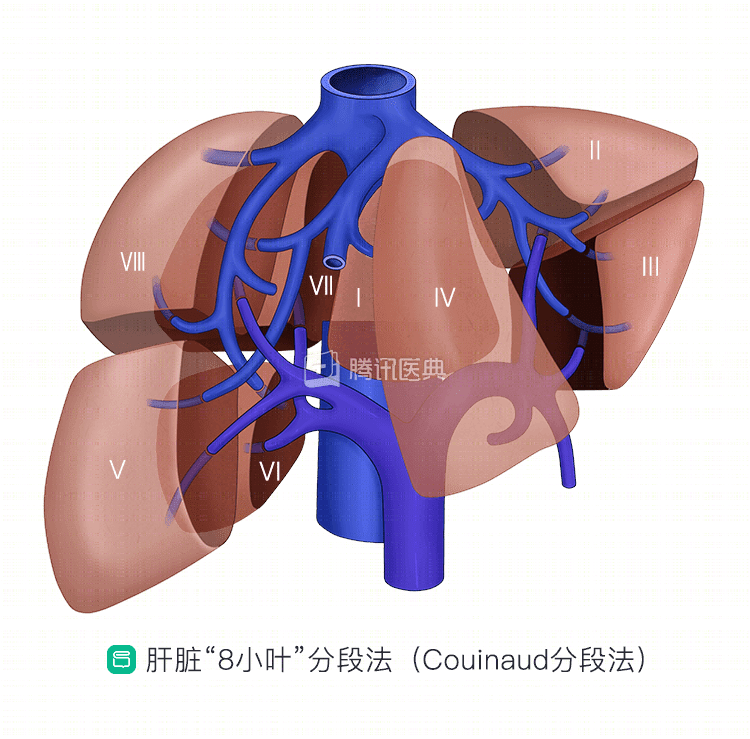
Anatomic hepatic segmental resection is based on the Couinaud liver segmentation method, which divides the liver into 8 functionally separate segments, each with matching inflowing blood flow, outflowing vessels, and bile ducts, with branches of the portal vein, hepatic artery, and bile ducts in the center of each segment and branches of the hepatic veins in the periphery of each segment.
Theoretically, anatomic resection based on liver segments can remove microscopic lesions that metastasize along the portal vein, thereby reducing recurrence after hepatectomy.
Characteristics of blood supply and metastasis in hepatocellular carcinoma
Blood supply characteristics of hepatocellular carcinoma include:
- Tumor blood supply is dominated by hepatic artery, but most have dual blood supply;
- Tumor microvascular structures show variable performance;
- Tumor nodules are surrounded by many small branches of the portal vein, one end of which communicates with the hepatic sinusoids and the other enters the tumor;
- Most portal venous branches enter the tumor and communicate with the tumor vascular plexus.
At different stages of tumor growth, the ratio of portal vein to hepatic artery blood supply differs. In the early stage of tumor, the portal vein is the main blood supply within the tumor, and as the tumor grows, the venous blood supply is gradually distributed to the tumor margin, and the center of the tumor is mainly supplied by the hepatic artery.
Cancer cells often spread along the portal vein, spreading and metastasizing in the liver, forming metastatic cancer nodules, which is the most important way of intrahepatic spread and metastasis in the early stage of hepatocellular carcinoma.
Based on the above characteristics of blood supply and metastasis of tumors, the main tumor and metastatic satellite foci in early metastasis of liver cancer are often located in the same liver segment, so anatomic hepatectomy can remove more microscopic metastases, thus reducing the postoperative recurrence rate and improving postoperative tumor-free survival and long-term survival.
Advantages of anatomic hepatic segmental resection
The goal of surgical resection of liver tumors is to effectively ensure tumor-free and safe margins of the main tumor and metastatic satellite foci and to ensure adequate postoperative residual liver.
Anatomic hepatic segmental resection can satisfy both of these by precise preoperative evaluation. The advantages are:
- The resection of liver segments according to the metastatic characteristics of the tumor can reduce postoperative recurrence;
- The segment-to-segment interface is relatively free of large vessels and bile ducts, so there is less bleeding in the section during resection, reducing postoperative complications such as bleeding and biliary fistula;
- Precise preoperative evaluation ensures adequate cut margins while maximizing the preservation of more liver tissue and reducing the likelihood of postoperative liver failure;
- Anatomic liver resection minimizes compression of the area where the tumor is located and avoids intrahepatic dissemination and metastasis due to cancer cell shedding.
Population for anatomic hepatic segmental resection
As research progresses, there is a consensus on the population for anatomic hepatic segmental resection:
- Tumors in the range of 2 cm to 3 cm.
- Anatomic segmental resection is more effective than non-anatomic segmental resection in reducing intrahepatic metastases when the tumor is 2 cm to 5 cm with good liver reserve and Child-Pugh class A.
- Anatomic hepatic segmental resection is not recommended for patients with tumors larger than 5 cm, Child-Pugh grade B liver function, more severe cirrhosis, and poor liver reserve function.
Of course, further validation in additional randomized controlled trials is needed to elucidate the true benefits and mechanisms of anatomic liver segment resection.