Once prostate cancer is diagnosed and the indication for radical prostate cancer surgery is met, patients and families should begin preparing for surgery.
What should I expect before surgery?
It is important to note that if a patient has been diagnosed with prostate cancer by transrectal puncture biopsy, it is best to wait 6 to 8 weeks after the biopsy before surgery to make the procedure less difficult, and 12 weeks after the biopsy for those who are about to undergo transurethral resection of the prostate.
In addition, medications such as aspirin, warfarin, and clopidogrel sulfate tablets (Bolivar) should be stopped for at least 1 week before surgery.
After you have been notified by the hospital that you are being admitted to prepare for surgery, you will often need to undergo a series of additional tests before surgery. For ease of understanding, these tests are divided into 3 categories:
- Routine tests that are required for any surgery: routine blood work, blood biochemistry, coagulation analysis, stool routine, urine routine, infection quadruple, chest X-ray, ECG, etc.
- Prostate cancer-related tests: MRI (most patients have had it before prostate puncture and can do without it), bone scan (to rule out bone metastases because patients with bone metastases cannot undergo surgery), etc.
- Other ancillary tests: Prostate cancer patients are mostly older men with relatively poor cardiopulmonary function, and echocardiography and pulmonary function tests may be performed as appropriate. In addition, a CO2 pneumoperitoneum machine is required to maintain pressure during laparoscopic surgery, resulting in increased partial pressure of CO2 in the patient’s blood circulation, and blood gas analysis can be performed preoperatively to assess the partial pressure of CO2 in the blood.
.
What other preparations are needed before surgery?
Most patients are very nervous before surgery, so please take a look at the table below and you will feel better about the surgery once you know what to expect.
| Time | Preparations |
|
|
| Preoperative |
|
| Day of surgery |
|
What is the procedure like?
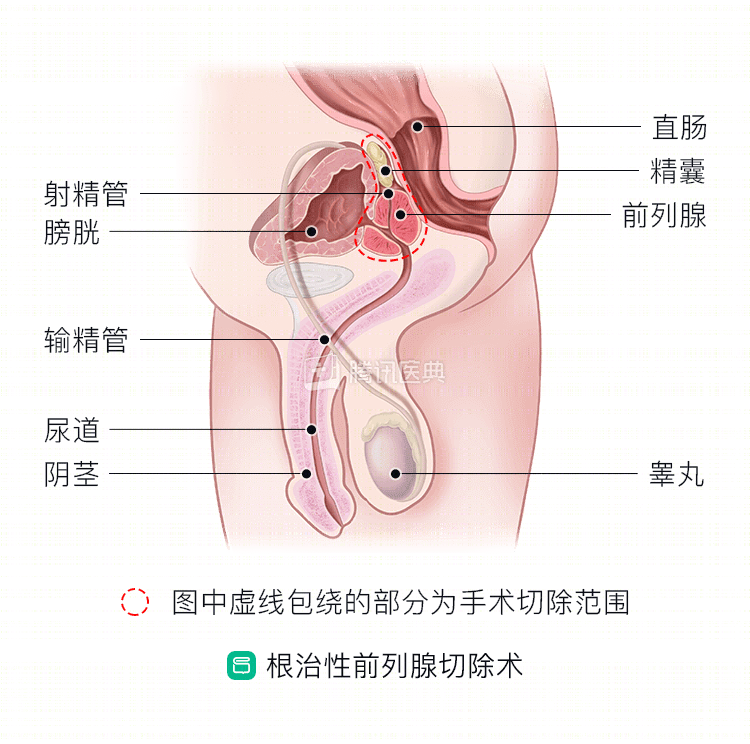
The surgical resection includes the complete prostate, bilateral seminal vesicles, and bilateral vas deferens jugular segments and bladder neck.
What are the possible risks of the procedure?
The current perioperative mortality rate is 0 to 2.1%, and the major complications can be divided into intraoperative and postoperative complications. Intraoperative complications that may arise include:
- Severe intraoperative bleeding: Bleeding due to injury to blood vessels during surgery.
- Rectal injury: The rectum is adjacent to the prostate and is at increased risk of rectal injury if the prostate is adherent to the rectum due to the cancer site.
- Pulmonary embolism: Occurs after deep venous thrombosis, when a venous thrombus breaks off and enters the pulmonary vasculature, blocking it with a large life-threatening thrombus. The risk of pulmonary embolism is higher in the elderly.
- Laparoscopic radical prostate cancer surgery may also have complications such as cancer metastasis along the incisional implantation, conversion to open surgery, gas embolism, and hypercapnia (because of the use of carbon dioxide pneumoperitoneum, which can occur if the surgery is prolonged).
Potential postoperative complications include:
- Erectile dysfunction: the incidence is 40% to 80%, resulting from intraoperative damage to the neurovascular bundle that controls erectile function.
- Deep vein thrombosis: Most often seen in high-risk patients. Advanced age, prolonged postoperative bed rest, and co-morbidities of certain medical conditions can lead to increased risk of venous thrombosis.
- Lymphatic cysts: Lymphatic cysts can result if lymphatic vessels are injured during surgery.
- Urinary fistula: If the vesicourethral anastomosis is poor, urine can leak through the anastomosis into the pelvis).
- Abnormal urination: The procedure may lead to urinary incontinence, vesicourethral anastomosis stricture, and urethral stricture.
Urinary incontinence is the most common postoperative complication
Postoperative incontinence is the most significant complication after radical prostatectomy. The normal voiding process in men requires a stable bladder forcing muscle, a functioning urethral sphincter, and normal innervation. Urinary incontinence after radical prostatectomy for prostate cancer is primarily associated with complete removal of the prostate and posterior urethra, resulting in significantly fewer structures to control urination.
Surgical approaches have been gradually improved to preserve the maximum amount of urinary control in patients. However, almost all patients continue to experience varying degrees of incontinence after removal of the urinary catheter, so always bring an adult diaper with you to outpatient follow-up visits for removal.
Variable degrees of urinary incontinence have been observed in the recent past after radical prostatectomy with removal of the balloon urinary catheter. If a patient is still unable to control urine properly 1 year after surgery, post-prostatectomy incontinence is diagnosed and requires professional help and appropriate treatment.
If incontinence occurs, pelvic floor muscle training (or anal lift) can be performed with training from your doctor and nurse, and within 1 year, most patients will have full control of urination with such training.
The method is to contract the abdomen, perineum, and anus simultaneously, holding your breath, for a total of 3 sets of 30 consecutive contractions each morning, noon, and night, with each contraction lasting more than 10 seconds.
The patient’s mastery of this exercise is assessed by the contraction force felt by the caregiver’s finger inserted into the patient’s anus. Of course, patients can also feel themselves, and if they feel a tightening sensation in the anus, this is a successful pelvic floor exercise.
How can I recover as soon as possible after surgery?
How to get well soon after surgery?
Although “early recovery” is everyone’s wish, we need to respect the objective rule that we should not be too anxious after surgery and try to cooperate with the medical staff.
Patient recovery instructions after surgery
| Post-op time | Precautions |
|
|
| 2 weeks after surgery |
|
| 2 months after surgery |
|