Nutritional support therapy for gastric cancer is aimed at patients with advanced gastric cancer in the peri-treatment (surgery, chemotherapy, radiotherapy) phase, home recovery phase, and those who develop malnutrition, through normal oral diet, enteral nutrition (oral, tube feeding), and parenteral nutrition (intravenous).
For those with good gastrointestinal function, the normal transoral diet route is easy to understand and is the best nutritional intake that physicians seek to achieve through treatment. However, during the treatment of gastric cancer, surgery, chemotherapy, and radiotherapy will affect the function of the gastrointestinal tract to varying degrees, especially surgery will change the structure of the gastrointestinal tract, damage the mucosa, and have a huge impact on metabolic and absorption functions, so other routes of nutritional support should be considered, mainly including enteral and parenteral nutrition.
Enteral nutrition (EN)
Enteral nutrition is a form of nutritional support that provides the body with nutrients such as metabolic requirements and other micronutrients through the still-functioning gastrointestinal tract. The physician will select the appropriate nutritional preparation based on a combination of disease conditions, surgical procedure, physical condition, nutritional status, gastrointestinal function, and risk of infusion, and may use many different routes of infusion.
- Routes of infusion The following routes of infusion are commonly used: oral, nasogastric, nasoduodenal, nasojejunal, gastrostomy, jejunostomy, etc. The most common routes of infusion for gastric cancer treatment are oral, nasogastric, nasojejunal, and jejunostomy tubes.

- Nutritional preparations The preparations in China’s market are mainly imported from Europe and the United States or joint ventures between European and American pharmaceutical companies in China. Since enteral nutrition preparations in Europe and the United States are registered according to medical foods, while China, Japan and other countries are registered according to drugs, the classification has not yet been unified. There are many kinds of nutritional preparations commonly used in China, and patients should choose suitable nutritional preparations and reasonable infusion routes under the guidance of doctors in gastrointestinal surgery, nutrition department, gastroenterology, etc.
- Infusion conditions The temperature, concentration, speed and input volume of the nutritional preparation are all required. Physicians usually control the temperature of the nutrient preparation at about 40°C, and gradually adjust the concentration from low to high, the speed from slow to fast, and the input volume from low to high, so that the gastrointestinal tract can gradually adapt and function back to a state of good absorption. Too concentrated, too fast or too much may cause the gastrointestinal tract to be unable to fully absorb and thus bloating and diarrhea may occur. Once the bloating and diarrhea persist, the doctor will make adjustments in concentration, speed and input volume, increasing or decreasing appropriately to achieve effective and optimal absorption of enteral nutrition.
- Infusion Methods Regular intermittent push, isometric incremental push, intermittent periodic gravity drip, and continuous pump-in drip are the 4 common infusion methods for enteral nutrition. The first 3 methods are subject to the principle of small amounts and many meals, and are generally administered 4 to 6 times per day at specific intervals to facilitate periodic gastrointestinal stimulation and to facilitate daily activities and examinations.
.
Usually enteral nutrition can be rapidly infused into the stomach, but the small intestine cannot tolerate rapid infusion and is prone to dumping syndrome, which is characterized by palpitations, tachycardia, sweating, vertigo, pallor, fever, weakness, and decreased blood pressure due to food entering the jejunum too quickly. The longer input time of cyclic drip facilitates speed control and improves infusion tolerance. The use of an infusion pump can effectively control the speed of input, the total amount of input, the amount of input per unit of time, and the completion of infusion, which can further improve the patient’s tolerance of enteral nutrition and facilitate management.
parenteral nutrition (PN)
Parenteral nutrition is the supply of nutritional elements, mainly fatty milk, amino acids, sugar, vitamins, electrolytes, and trace elements, to patients through the intravenous route, and the complete parenteral nutrition is called total parenteral nutrition (TPN). The total parenteral nutrition is called total parenteral nutrition (TPN). Parenteral nutrition can be supported by both peripheral and central venous routes.
- Parenteral nutrition via peripheral veins This route is indicated in the following situations.
- Short-term parenteral nutrition (no more than 2 weeks), where the osmolality of the nutrient solution is less than 1200 mOsm/LH2O;
- Central venous line placement is contraindicated or not feasible;
- Patients with catheter infection or sepsis.
This method is simple and easy to use, avoids mechanical problems, infection and other complications associated with central venous placement, and allows for easy early detection of phlebitis, but has the disadvantage that the infusion osmolarity cannot be too high, requires repeated punctures, and is prone to phlebitis. Therefore, long-term use is not advisable.
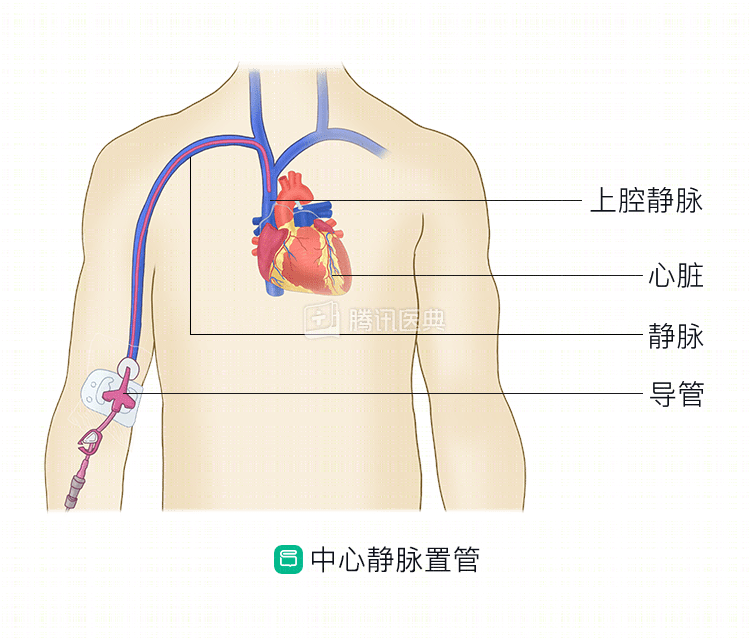
- Parenteral nutrition via central vein This route is indicated for parenteral nutrition for more than 2 weeks with an osmolarity above 1200 mOsm/LH2O.
Placement routes include access to the superior vena cava via the internal jugular vein, subclavian vein, or peripheral veins of the upper extremity. The central venous line can be placed subcutaneously with a catheter for infusion, also known as a Catherter-Port, which can be left in place for a long period of time and does not interfere with the patient’s daily life such as bathing and socializing, which can improve the patient’s quality of life and has been used more often in the clinic.
Tips
Several routes of nutritional support therapy for gastric cancer have their own advantages and disadvantages for different situations, and the order of choice in treatment is transoral diet, enteral nutrition, and parenteral nutrition. However, in the clinical practice of nutritional support therapy, a single pathway often cannot meet the target requirement of nutritional support, and the professional committee of tumor nutrition and supportive therapy of Chinese Anti-cancer Association recommends the combined application of diet, enteral nutrition, and parenteral nutrition, i.e., part diet + part enteral nutrition + part parenteral nutrition . (Contributed by Peng Deng, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)