The location of the esophagus is deep, with a rich blood supply and a rich network of lymphatic vessels in the submucosa; therefore, radical surgery for esophageal cancer is complex and prone to various postoperative complications, and the choice of surgical approach requires a comprehensive assessment of many factors:
- Tumor location, length, depth of submucosal spread, and adhesions of the tumor to surrounding structures;
- The extent of lymph node dissection planned;
- The choice of replacement esophageal organ;
- Surgeon’s preference.
Different sites of esophageal cancer with different approaches to resection and reconstruction
The esophagus is approximately 25-30 cm long, extending from the level of the 7th cervical vertebra to the 11th thoracic vertebra, and is divided into cervical, thoracic, and ventral segments (as shown in the figure).
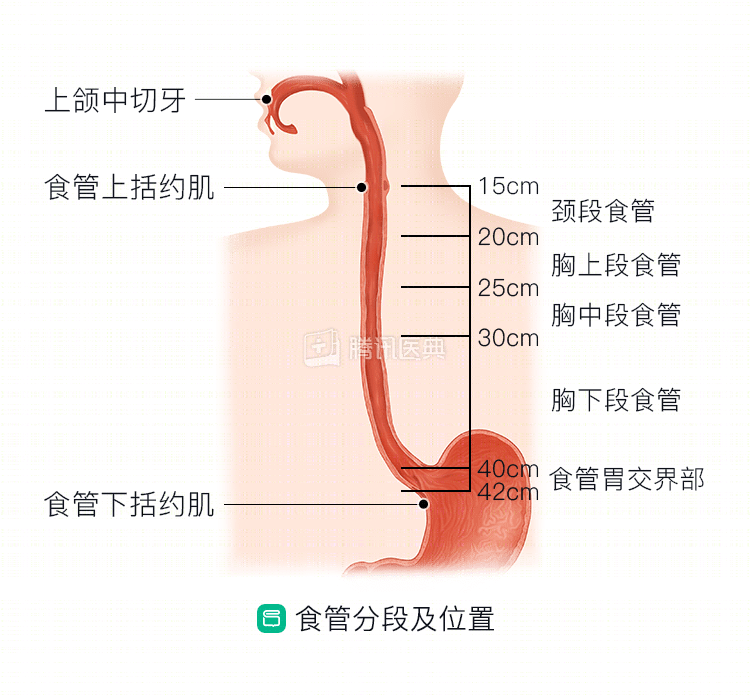
Neck segment
The location is unique, and surgery is risky and can easily injure the “innocent” larynx and trachea, so chemotherapy and radiation are usually preferred. If you don’t want to do radiotherapy, or if you don’t get good results after trying radiotherapy, you can also have surgery to remove it.
Surgical approach:
Usually a portion of the pharynx and larynx is removed, and the distal trachea may require a permanent stoma (i.e., a soft material that is made to resemble the trachea). Intraoperative clearance of bilateral supraclavicular region lymph nodes is often required. The surgeon will also lift the stomach in place of the esophagus and anastomose it with the pharynx to reconstruct the upper gastrointestinal tract.
Tumors that are confined to the upper cervical esophagus are a bit out of reach to lift the stomach. This is a very traumatic procedure, and on the other hand, there is no way to guarantee your quality of life after surgery. The doctor will often take a piece of tissue from the jejunum or the deltoid or pectoralis muscle of the chest and anastomose it to the removed part of the esophagus, cleverly “transposing” it to avoid the esophageal stump.
Thoracic segment
When a tumor invades the thoracic esophagus, there may be a risk of “jumping metastases” in the submucosa. This is a relatively unique feature of esophageal cancer, for example, thoracic esophageal cancer may “jump” to the abdominal or cervical lymph nodes rather than metastasize “close” to the chest lymph nodes. Therefore, the physician will focus on whether the lymph node clearance is clean.
Currently, the National Comprehensive Cancer Network (NCCN) recommends the following radical surgery for esophageal cancer:
- Left cervical-right thoracic-abdominal triple-incision esophagectomy (McKeown procedure);
- Two-incision trans-right thoraco-abdominal esophagectomy (Ivor-Lewis procedure);
- Two-incision trans-right thoraco-abdominal esophagectomy (Ivor-Lewis procedure)
- Esophagogastrostomy through the esophageal fissure (non-open approach);
- minimally invasive robotic esophagogastrectomy (minimally invasive procedure);
- Intrathoracic or cervical anastomosis with left-sided transthoracic or combined thoracoabdominal approach.
These procedures are very specialized; all you need to know is that everything changes and they all consist of 3 core components: esophagectomy, tubular gastric production, and anastomosis of the residual esophagus and tubular stomach. Opening the right chest facilitates exposure of the entire thoracic segment of the esophagus and is now used more often; opening the left chest is indicated for partial lower segment esophageal cancer, which can avoid the obscuration of the diseased esophagus by the heart and aortic arch and cut off as much length as possible.
Today, there are many “evolutions” of these procedures, and the “weapons” are more advanced, with the use of thoracoscopy and laparoscopy to perform minimally invasive surgery, and more advanced robotic-assisted surgery.
I hope you understand that there are no absolute advantages or disadvantages to the next procedures, and that your thoracic surgeon will choose the most appropriate procedure for you on a case-by-case basis.
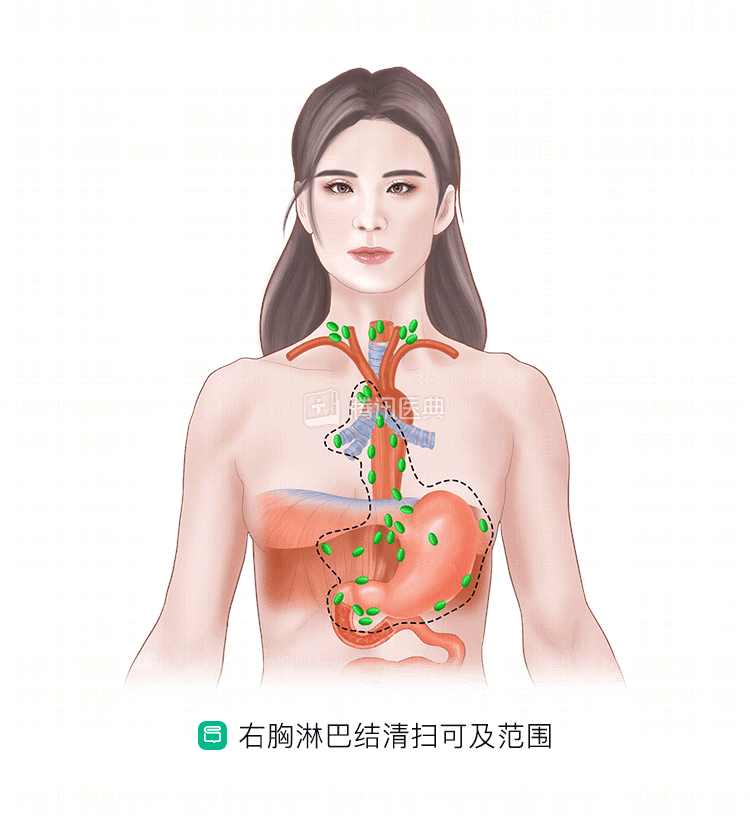
1. Mckeown surgery and Ivor Lewis surgery for right thoracic approach: lymph node dissection is complete and can be minimally invasive using thoracoscopy or robotics
Right thoracic surgery is indicated for lower esophageal cancer and adenocarcinoma of the esophagogastric junction. It is characterized by ease of exposure, resection of esophageal lesions, and greater lymph node clearance than left thoracic surgery (below).
When it comes to surgery, the first reaction of most patients and families is: is it invasive and can it be minimally invasive?
I want to make it clear that the combined thoraco-laparoscopic Ivor Lewis procedure is now the procedure of choice in most tertiary care hospitals. It is also known as “keyhole surgery,” with incisions ranging from 4-5 cm to 0.5-1.0 cm. Through these small incisions, the surgeon can perform lumpectomy to clear the abdominal cavity and mediastinal lymph nodes, as well as create and anastomose the “tubular stomach. The postoperative incision is mildly painful. The postoperative incision is mildly painful, and you will recover quickly.
2. Transesophageal fissure resection: no chest opening, less traumatic, suitable for people of advanced age and poor cardiopulmonary function
The biggest advantage is that the procedure is less invasive and does not open the chest, which is especially suitable for those who have difficulty tolerating greater surgical trauma, such as those of advanced age and poor cardiopulmonary function, as well as those with early lesions and no lymph node metastases. It can be well resected for tumors of lower esophagus and gastroesophageal junction, as well as high-grade cervical esophageal cancer. The drawback is that it cannot completely clear the lymph nodes.
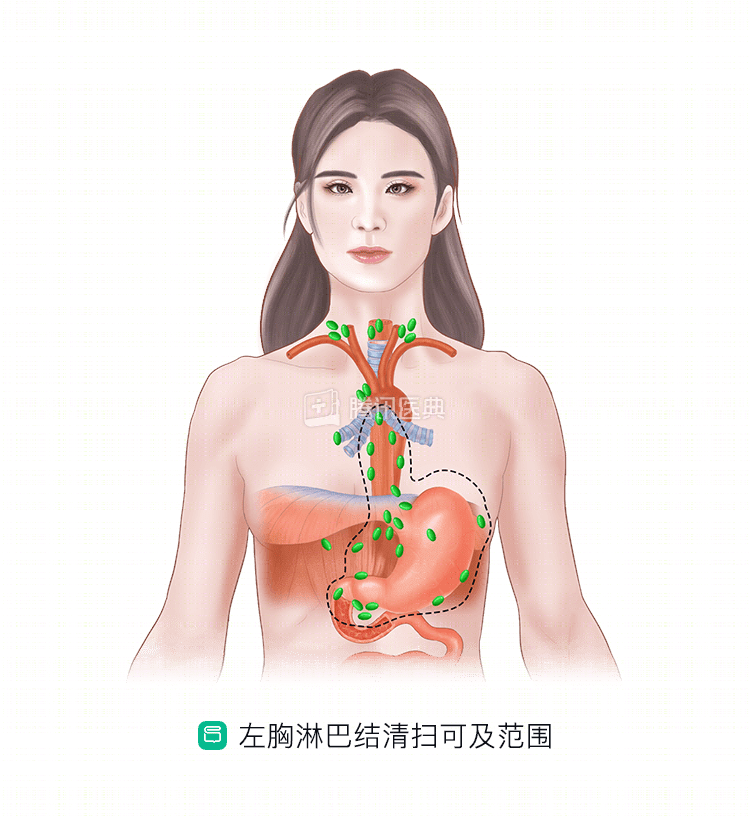
3. Left thoracic approach: less invasive, easy to switch chest, improved and enhanced in China
Medically known as the “Sweet procedure,” it is the oldest surgical approach for esophageal cancer. But in the 1970s, even in Japan, which has some of the best surgical data in the world, the mortality rate was as high as 20%, and the 5-year survival rate for patients was only 12%. Causes include anastomotic fistula, pulmonary complications, and circulatory collapse.
With improved technology, the mortality rate for esophageal cancer surgery with a predominantly left thoracic approach in China has decreased to about 2%, and the survival rate has increased to 20% to 30%. Therefore, in China, left thoracic surgery is still the first choice for many surgeons.
Why do we go to great lengths to improve left-sided thoracic surgery? Because it has some advantages: it provides good exposure of the middle and lower esophagus, the left diaphragm, the aorta, and the stomach and spleen in the left epigastrium; it is less invasive, better tolerated by the patient, and easy to switch the chest on and off.
Of course, compared with the right thoracic approach, the left thoracic procedure is still very limited in terms of the extent of bilateral upper mediastinal lymph node dissection (as shown above).
Ventral segment
For tumors that occur at the junction of the esophagus and stomach or in the intra-abdominal esophagus, partial esophagectomy and gastrectomy or extended gastrectomy is usually performed. This type of surgery sometimes requires an open chest and sometimes does not require an open chest.
Regardless of the method of resection, radical (R0) resection, resection distal to 4 cm from the stomach, resection proximal to 5 cm from the esophagus, and resection of at least 15 lymph nodes draining the primary tumor area are necessary. These, of course, are also judged by the surgeon on an intraoperative basis.