Recurrence of metastasis after esophageal cancer treatment is a hurdle for many patients to face. This means that the disease is advanced and treatment is more complex. Doctors will consider the way the tumor has progressed (local recurrence, or distant metastasis), the number and size of metastases, general physical condition, and the time it took to control the disease after initial treatment to develop a treatment plan.
In this article, we look at the development of a treatment plan for recurrent metastases after surgery for esophageal cancer through a case study.
Mr. Jiang, 62, developed a choking sensation when eating in November 2012, which was more pronounced when eating harder solid foods and got progressively worse.
First treatment
Mr. Kang went to the hospital for various tests, including gastroscopy and pathology, and was diagnosed with squamous carcinoma of the upper thoracic esophagus, clinical stage II.
He received two cycles of paclitaxel + cisplatin regimen chemotherapy (neoadjuvant chemotherapy) followed by radical esophageal cancer surgery.
Post-operatively, Kang has recovered well and his regular review results have been excellent.
Recurrent disease
After 4 good years, Kang developed hoarseness in 2016, which gradually worsened. He rushed back to the hospital to get checked out.
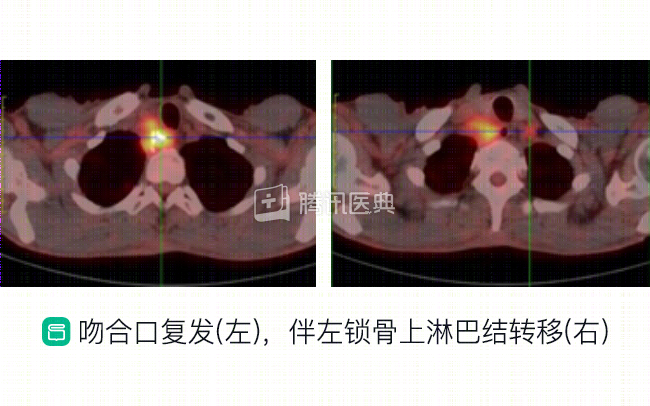
PET-CT results showed a new mass at the surgical anastomosis with enlarged left supraclavicular lymph nodes.
After learning of the recurrent metastasis, Jiang felt like the sky was falling. The doctor provided him with timely psychological counseling.
The doctor said:
Recurrence of esophageal cancer after surgery is relatively common. After the diagnosis of recurrence, it is important to adjust the mentality and treat actively, and most patients can benefit.
Second treatment
The doctors believe that Mr. Kang had chemotherapy before his initial surgery and that it worked well, so this treatment is still a 2-week chemotherapy as an “emergency”.
After chemotherapy, he had some adverse reactions, with nausea and vomiting being particularly evident. The blood tests showed that both white blood cells and platelets were lower.
The doctor said:
Nausea and vomiting are common side effects of chemotherapy. Don’t worry too much about them, they will go away with symptomatic treatment. Your doctor will evaluate your body before treatment and only if the conditions are met will chemotherapy be administered, so it will not affect the efficacy of the treatment.
Mr. Kang insisted on completing the treatment. The follow-up evaluation found that the tumor had shrunk from 17mm to 12mm.
The internal medicine and radiation therapists consulted and concluded that continued radiation therapy would further control the disease and prolong survival. After a comprehensive evaluation, Mr. Kang had no contraindications to radiotherapy, was effective with chemotherapy, and was in good health to be given concurrent low-dose chemotherapy with radiotherapy for sensitization.
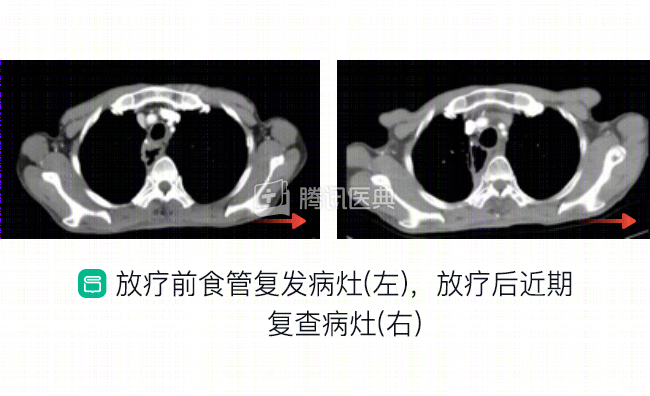
Next, Mr. Kang completed 30 radiation treatments and had 6 weeks of “paclitaxel + cisplatin” weekly chemotherapy.
At about the 20th radiation treatment, he developed significant swallowing pain, and it was painful to swallow saliva, so he asked his doctor about it.
The doctor said:
Sore swallowing is a common side effect of radiation therapy for esophageal cancer, and tends to be most pronounced around 20 radiation treatments. Direct injury from radiation therapy and the edema and inflammation it causes are causes of pain that can be reduced with symptomatic treatment. It will slowly recover about 1 month after the end of radiotherapy. It is recommended to try to adhere to the completion of radiotherapy, and interruption of radiotherapy will make the efficacy of the treatment much worse.
Mr. Kang insisted on completing his entire radiation treatment plan. He was reviewed every 3 months after treatment was completed. So far, the disease is satisfactorily controlled.
Summary
Currently, stage I, II, and III esophageal squamous carcinoma is treated with a combination of mainly surgical procedures, but the outcome of surgery alone is unsatisfactory, with more than half of patients experiencing recurrence of metastasis within 5 years after surgery. The results are usually the reappearance of choking sensation, pain, hoarseness, etc.
Neoadjuvant chemotherapy and neoadjuvant radiotherapy before surgery, as well as adjuvant radiotherapy after surgery, can significantly prolong patient survival and reduce the likelihood of recurrent metastases.
PET-CT is a common tool for confirming recurrent metastases. Doctors often use the metric SUV max (SUV maximum), which represents the level of glucose metabolism of cells at the lesion; the higher the value, the more active the malignant cells. In general, a SUVmax >2 means a high likelihood of malignancy.PET-CT can also show the size of metastatic lymph nodes. In general, the larger the short diameter, the greater the likelihood of malignancy, >1 cm is considered a metastatic lymph node.
Patients who present with recurrent metastases after surgery, or who are stage IV at diagnosis, are often lost to surgery and are treated mostly with radiotherapy and chemotherapy. In particular, radiotherapy is more effective in controlling recurrent metastases, and the combination of chemotherapy can have a “sensitizing” effect.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from a competent physician regarding your specific treatment plan.
Co-authors: Dr. Dong Dezuo Dr. Zhang Yangzi, Department of Radiotherapy, Peking University Cancer Hospital