Renal cancer vena cava tumor thrombi are neoplastic organisms that form in the lumen of the inferior vena cava vessels where the tumor extends from the primary site in the kidney. The tumor thrombus originates in the vein where the tumor is located and extends into the renal vein, the inferior vena cava, and even the right atrium and right ventricle. Most of the tumor thrombi extend along the lumen of the vein and some invade the vein wall.
The classification of vena cava thrombi in renal cancer is based on the Mayo Medical Center’s five-level classification:
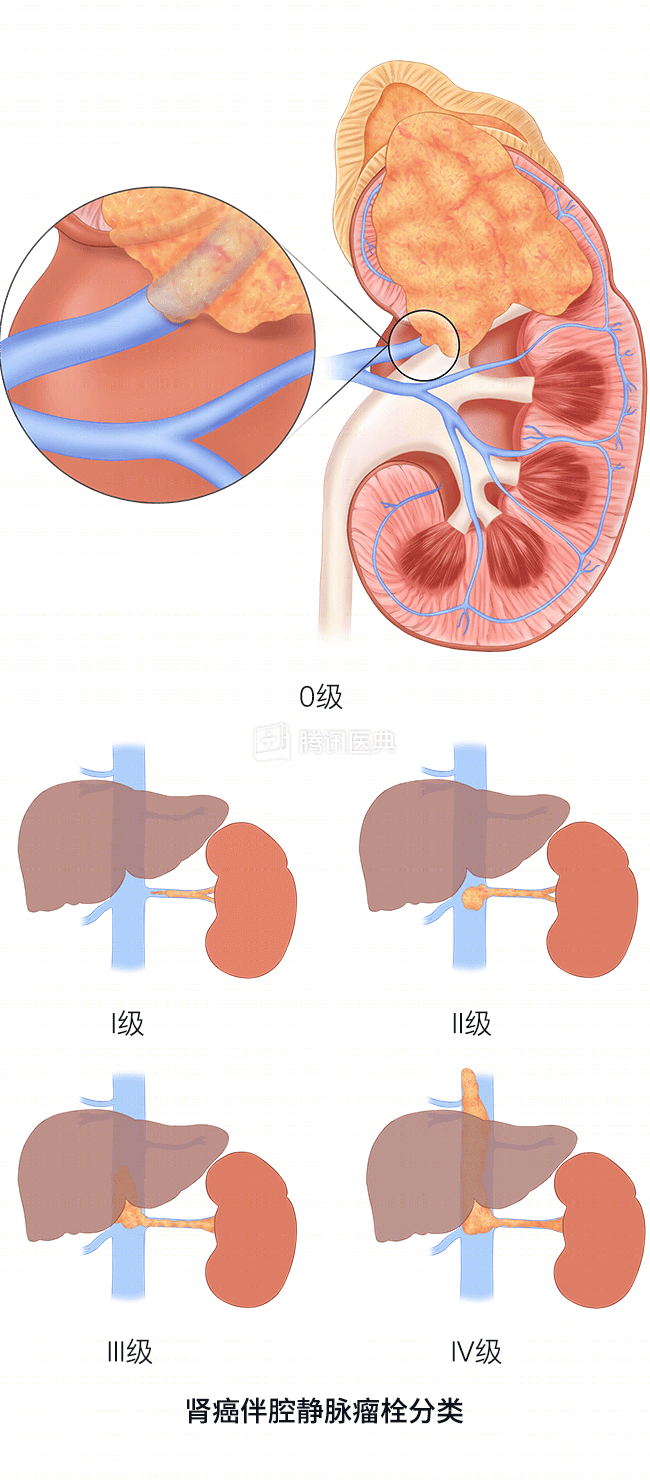
- Grade 0
- Grade 0: the tumor is confined to the renal vein;
- Grade I: invasion of the inferior vena cava with the tip ≤2 cm from the opening of the renal vein;
- Grade II: apical part of the tumor is 2 cm from the opening of the renal vein, but below the level of the hepatic vein;
- Grade III: the growth of the tumor embolus reaches the level of the inferior vena cava in the liver, but below the level of the diaphragm;
- Grade IV: tumor thrombus invades the inferior vena cava above the level of the diaphragm.
How is it diagnosed?
- MRI is one of the most sensitive means of detecting vena cava tumor emboli and can also characterize the highest level of emboli.
- Intraoperative ultrasound can help the surgeon find and locate the tumor embolus intraoperatively.
- While CT scans can visualize tumors, only the most advanced CT can provide anatomic detail of tumors.
How is it treated?
Kidney cancer with thrombus.
Kidney cancer with tumor emboli usually requires open surgical resection and is usually done on the basis of a radical nephrectomy.
Laparoscopic surgery is generally indicated only in cases where the thrombus is confined to the renal vein and not in cases of inferior vena cava thrombosis.
The resection of an aneurysm depends on the height of the aneurysm, and the surgeon must specify the level of the aneurysm.
- If the highest level of the inferior vena cava embolus does not exceed the diaphragm, then the surgeon wishes to complete the procedure without the need for extracorporeal circulation and opening the chest cavity;
- Once the level of the tumor embolus exceeds the diaphragm (or even reaches the right atrium), then the surgery becomes extraordinarily complex and risky, at which point surgical resection is accomplished through the combined efforts of urologic, cardiothoracic, vascular, and anesthesiologic specialists.
For these patients with tumor thrombus levels above the diaphragm and very high surgical mortality, preoperative pharmacologic therapy is administered, and if the tumor can regress below the level of the diaphragm after treatment, the complexity of the surgery will be significantly reduced.