We know that surgery is expected to cure esophageal cancer, but surgical treatment has strict indications. Surgery is not the first choice for those with significant local outward tumor invasion, excessive number of lymph node metastases, the presence of distant metastases, and the presence of severe medical disease.
But this group of patients is not “hopeless”. In order to try to cure the tumor, doctors may consider simultaneous radiotherapy. In this article, we present a case study to show how a concurrent radiotherapy regimen is developed.
Insurgable locally advanced esophageal cancer
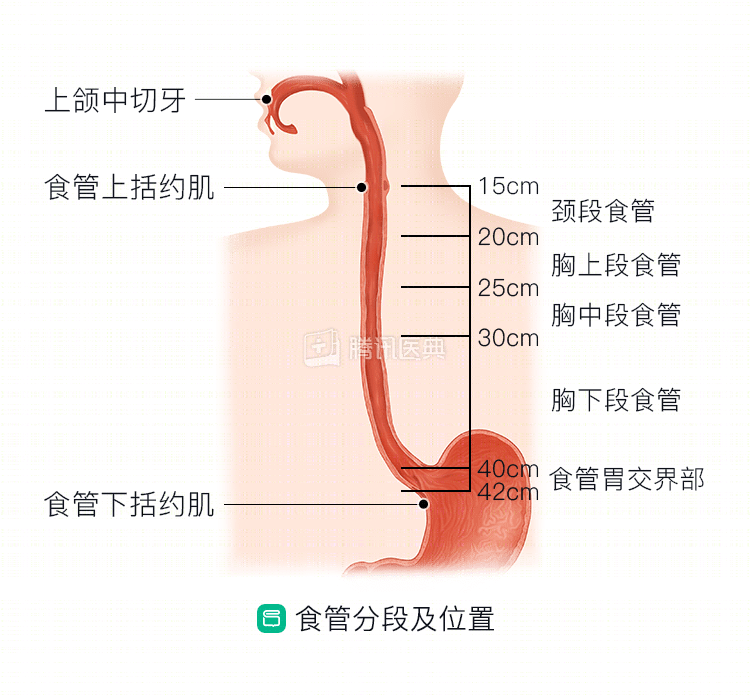
Mr. Peng, 61, presented with progressive dysphagia in February 2016. At his initial visit, he was already limited to a liquid diet and had lost 4 kg in 1 month. gastroscopy and pathology suggested a moderately differentiated squamous carcinoma in the mid-thoracic segment of the esophagus.
Mr. Peng came to Peking University Cancer Hospital and after perfecting the examination, it was found that the tumor had invaded the aorta and metastasized to several lymph nodes, but there were no distant metastases yet. The doctors judged it to be locally advanced, inoperable, and poorly treated with radiotherapy alone. Since there were no deep ulcers in the esophageal wall, the risk of esophageal perforation was low, and it was decided to try simultaneous radiotherapy in order to strive for a radical cure.
Treatment procedure
Pre-treatment preparation
At the time of admission, Mr. Peng had already experienced significant weight loss and was only able to eat a liquid diet. And after starting synchronous radiotherapy, radiation esophagitis may occur, affecting eating, aggravating malnutrition, and even preventing completion of treatment. Therefore, doctors placed a gastric tube prophylactically before treatment to ensure nutritional intake.
The risk of radiation pneumonia during radiation therapy is higher because of long-term smoking. Therefore, doctors advised Mr. Peng to quit smoking immediately.
Treatment process
Radiotherapy
Treatment schedule: Outpatient, 8 to 10 minutes per week 5 times a week (Monday through Friday), with weekends off, for 5 to 6 weeks.
Technology: Volumetric modulated arc radiotherapy (VMAT), which allows for “precision radiotherapy” by giving different doses to different areas in the same session.
Range of irradiation: primary cancer, tracheoesophageal groove, and mediastinal metastatic lymph nodes.
Ranges: 60 Gorey (Gy)/50.4 Gorey (Gy)/28f (28 sessions in total). Of these, a 60 Gy dose was used for lesions clearly identified on imaging films and a 50.4 Gy dose was used for areas that were not visible on imaging films but may have tumor invasion.
Chemotherapy
Treatment schedule: 1 day per week inpatient infusion chemotherapy for 5 sessions,
Protocol: paclitaxel + cisplatin.
Adverse effects and response
After 8 radiation treatments, Mr. Peng began to have painful swallowing but was able to eat fluids. He also had mild malaise and reduced white blood cells and neutrophils. He was very anxious and wanted to do only radiation therapy.
The doctor reassured him that painful swallowing was common and that most of it would go away after treatment was over, so there was no need to worry too much. The other side effects are mild, and it is safe to continue with concurrent radiation and chemotherapy. The doctor also said that the pain was not a problem, and that the pain was not a problem.
The doctor advised him to drink only a small amount of water for now and to avoid eating through the mouth. The energy supply was ensured by infusion of nutritional fluid or homemade vegetable juice and milk through a gastric tube. Pain-relieving and esophageal mucosa-protective medications were also prescribed.
Since then, his pain has gradually improved. He was able to eat a small amount of liquid food by the time he had 20 sessions of radiation therapy and eventually completed all of his treatment.
Post-treatment follow-up
One month after treatment, Mr. Peng returned to the hospital for a follow-up. By this time, his painful eating symptoms were significantly relieved, he was able to eat porridge, vegetable puree, and minced meat, and his weight was back to what it was before he became ill.
A repeat upper gastrointestinal tract imaging showed that the mass was mostly gone. Chest CT showed a reduction in ductal wall thickening and a reduction in mediastinal lymph nodes.
The outcome was evaluated as a partial response (PR).
Since then, Mr. Peng has maintained the habit of regular review every 3 months. No recurrence has been detected for 2 years now, and he has been able to eat a regular soft diet.
Summary
Synchronous radiotherapy is the current standard of care for unresectable, locally advanced esophageal cancer.
After the completion of concurrent radiotherapy, most patients are expected to achieve a “radical” outcome.
Most people will develop radiation esophagitis after more than 10 radiation treatments. If a gastric or jejunal tube was not placed prior to treatment, aggressive intervention is needed with local symptomatic management, intravenous nutritional support, and in severe cases, adjustment of chemotherapy medications may be considered as appropriate.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a “like patient” treatment decision. Please seek professional advice from a competent physician regarding your specific treatment plan.
Co-Author: Dr. Yangzi Zhang, Peking University Cancer Hospital