The overall recurrence rates of esophageal cancer 1, 3, and 5 years after surgery are 28%, 44%, and 64%, respectively, and local recurrence rates can reach 17%, 27%, and 43%, respectively. Its postoperative recurrence and metastasis can be divided into local recurrence and distant metastasis. Depending on the location and stage of the tumor, the sites prone to recurrent metastasis and the possible symptoms are also different.
Local recurrence
The types of local recurrence include: regional lymph node metastasis, anastomotic recurrence, and recurrence in the original tumor bed.
Lymph node metastasis
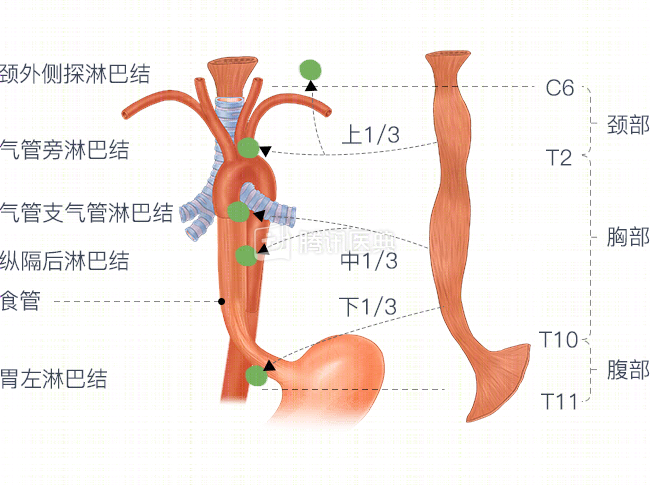
Mediastinal lymph nodes are the most common site of lymph node metastasis in esophageal cancer, accounting for 62.9% to 80.2%.
The mediastinum is a separate space within the thoracic cavity, which contains a large number of important organs, such as the thymus, trachea, esophagus, heart, and aorta, as well as many nerves and lymphatic ducts and lymph nodes.
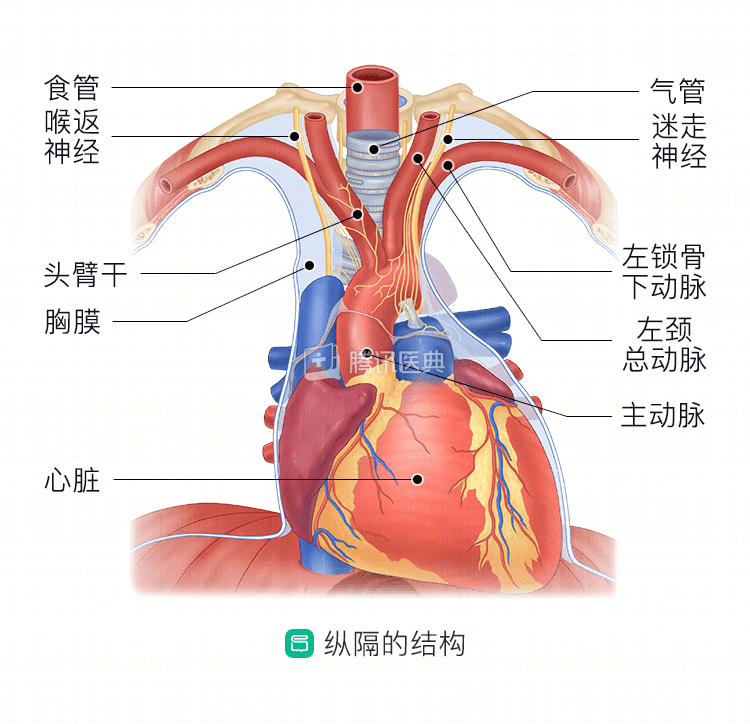
The upper mediastinum contains a variety of large vessels and nerves, which make lymph node dissection difficult and prone to incomplete dissection, and then regional lymph node recurrence and metastasis may occur, mainly including cervical and mediastinal lymph nodes.
Metastases to cervical lymph nodes may present as a neck mass; mediastinal lymph node metastases often have no specific clinical presentation and are usually detected by periodic review of chest CT.
When a locally recurrent tumor invades surrounding tissue structures, symptoms such as hoarseness, Horner syndrome (also called “cervical sympathetic syndrome” or “Horner’s syndrome”), which is characterized by miosis, ptosis, and The syndrome is also called “cervical sympathetic syndrome” or “Horner’s syndrome,” which is characterized by narrow pupils, droopy eyelids and narrow fissures, and sunken eyes.
Anastomotic recurrence
Esophageal cancers of the cervical and upper thoracic segments, or multiple primary esophageal cancers (MPEC), are prone to local recurrence of the anastomosis after surgical resection. Among them, MPEC is a special type of esophageal cancer, which refers to the occurrence of two or more primary malignant tumors in different parts of the esophagus simultaneously or sequentially. The incidence of MPEC in the population of esophageal cancer is 9.5%~32.2%, and radical surgery and radiotherapy are mostly chosen according to clinical stage, tumor site, and systemic condition.
Recurrence in the original tumor bed
Esophageal cancer patients with tumor pathological stage of T3 and T4 are prone to local recurrence of the original tumor bed due to tumor infiltration and outgrowth and increased possibility of occult tumor residual.
Distant transfer
Distant metastases include, non-regional lymph node metastases and other organ metastases.
Non-regional lymph node metastases
These include metastases to the abdominal cavity and retroperitoneal lymph nodes. They are often detected by abdominal CT and in severe cases may show signs of pneumoperitoneum.
Metastasis to other organs
Distant metastases from esophageal cancer are most likely to reach the liver and may present with epigastric pain, loss of appetite, postprandial epigastric fullness, nausea, vomiting, and diarrhea, as well as low-grade fever, wasting, weakness, jaundice, edema, bleeding from the gums, nose, and subcutaneous petechiae.
In second place are the lungs. Because of the less frequent presence of bloody sputum, the early symptoms of esophageal cancer lung metastases are not obvious, and only when the tumor progresses to a certain level does it compress the surrounding structures and produce symptoms or pain. The lung metastases from esophageal cancer are usually detected during regular review of chest CT, which requires you to follow your doctor’s instructions for regular review after surgery.
In addition, metastases may occur in organs such as bone, brain, adrenal glands, and pleura, and you may experience bone pain, neuropsychiatric symptoms, low back pain, and pleural effusion.
We hope you will insist on a close postoperative follow-up to detect possible recurrence and metastasis as early as possible to avoid missing the best time for treatment.