Laparoscopic surgery is a minimally invasive procedure, and gastric cancer surgery is seen as a “major surgery” by many patients. Even for the “major surgery” of gastric cancer surgery, in many cases it can be accomplished through minimally invasive laparoscopy. This article takes a look at how laparoscopy can be used to perform gastric cancer surgery.
Preparation: general anesthesia
Like gastric cancer surgery, laparoscopic surgery requires tracheal intubation under general anesthesia. For the patient, the procedure is complete after a “nap,” and there is no difference in how the patient feels about the two procedures.
What is the procedure like?
What is the procedure like?
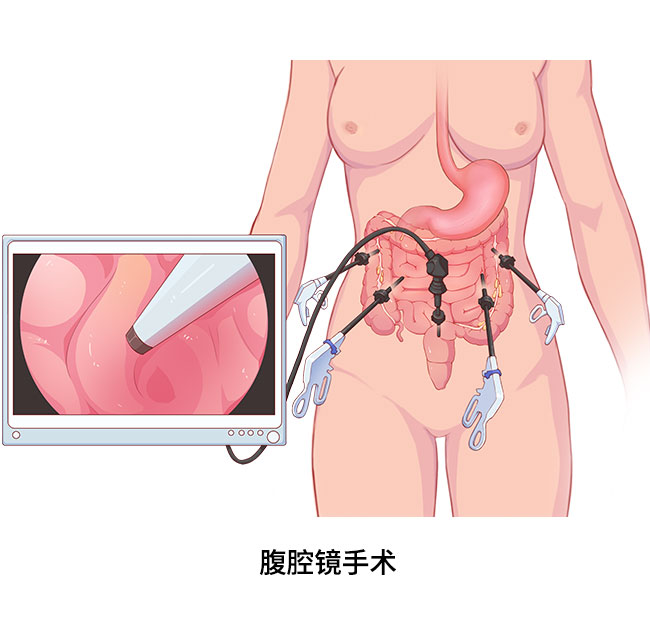
Unlike surgery, laparoscopic surgery does not require an extensive incision of the abdominal wall, but rather the creation of several 0.5- to 1.0-cm holes in the abdominal wall where high-definition or 3D laparoscopic lenses are placed to display images of the abdominal cavity on a monitor screen. These lenses are the equivalent of the surgeon’s eyes, allowing observation of the abdominal cavity.
The surgeon also places special laparoscopic instruments through holes in the abdominal wall, through which the entire procedure is performed.
It is important to note that during laparoscopy, the surgeon continuously injects carbon dioxide gas through the hole in the abdominal wall, which itself is harmless to the patient and does not add additional sensations after the procedure, in order to prop up the abdominal wall with gas and create space for the laparoscopy.
Some patients wonder how the excised gastric cancer tissue can be taken out when the hole is so small. The surgically resected specimen can be removed through a very small abdominal wall incision under the good protection of specially designed materials. Depending on the extent of the surgical resection and the specific laparoscopic procedure, the size of the incision varies from about 6 cm, much smaller than the traditional open incision.
The principles of surgery are no different from surgery
Like surgery, laparoscopic surgery for gastric cancer follows the same principles of asepsis and tumor-free operation, meaning that the surgeon will avoid contamination from intraoperative manipulation and avoid the development of metastatic tumor implants. For patients who meet the indications, there is no difference between laparoscopic surgery and open surgery in terms of the extent of lesion removal and lymph node dissection.
What are the characteristics of laparoscopic surgery?
The unique advantage of laparoscopic surgery is that it facilitates either a purely exploratory laparotomy, which is an exploration of the abdominal cavity without management of the tumor, or an exploratory laparotomy at the beginning of the laparoscopic procedure. Through laparoscopic exploration, the surgeon can observe the situation inside the abdominal cavity without cutting into the abdominal wall and find out many problems that are difficult to be clarified by imaging before surgery, such as peritoneal implant metastasis, metastasis to other organs in the abdominal cavity and intra-abdominal adhesions, which can help the surgeon to decide whether to switch to open surgery or stop the surgery in the middle of the operation. Laparoscopic exploration avoids the trauma associated with traditional open exploration and facilitates the patient’s rapid postoperative recovery. In addition, some cells can be collected for exfoliative cytology during laparoscopic exploration, which can help to better determine the stage of disease and guide treatment such as neoadjuvant therapy and peritoneal perfusion chemotherapy.
In terms of gastric cancer surgery, traditional open surgery often requires a large abdominal wall incision, whereas laparoscopic surgery requires only a small incision to remove the resected tissue specimen. Thus, laparoscopic surgery has the advantages of reduced trauma and bleeding, less postoperative pain, less incisional scarring and incisional complications, and faster postoperative recovery.
However, laparoscopic surgery also has some shortcomings. Because of the complex anatomy of the stomach and the presence of more complex and variant blood vessels, it is more difficult to perform gastric cancer surgery laparoscopically. Early laparoscopic gastric cancer surgery is mainly used to treat early stage gastric cancer and has achieved long-term outcomes comparable to those of conventional surgery. Today, studies have confirmed that for progressive gastric cancer, laparoscopic surgery has advantages over open surgery in terms of near-term outcomes (e.g., bleeding, postoperative incisional pain, risk of incisional infection, length of hospital stay), comparable long-term outcomes, and can be performed safely and effectively by experienced surgeons in large medical centers. Although current studies suggest that laparoscopy can perform standard radical surgery for gastric cancer, laparoscopic surgery is still contraindicated in patients with gastric cancer requiring expanded lymph node dissection.
Laparoscopic surgery has its own unique indications and surgical complications, and there is also the possibility of requiring intermediate open surgery.
Because laparoscopy has the advantages of smaller incisions, less trauma, less postoperative pain, and faster recovery, it also has the disadvantages of more limited indications and more complex complications. Therefore, laparoscopic surgery is not suitable for all gastric cancer patients, and doctors will make individualized recommendations based on patients’ conditions and their own wishes. (Coauthored by Hanyu Chen, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)