As the general population takes medical examinations more seriously, more and more cystic kidney lesions are being found. The most important thing is that the cystic lesions are not found in the kidney. The most important thing is how to distinguish between kidney cancer and cysts, because my attitude is “don’t let it go, don’t catch it wrong”.
Let’s first recognize the characteristics of each of kidney cancer and kidney cyst:
| Kidney cancer | Renal cysts | |
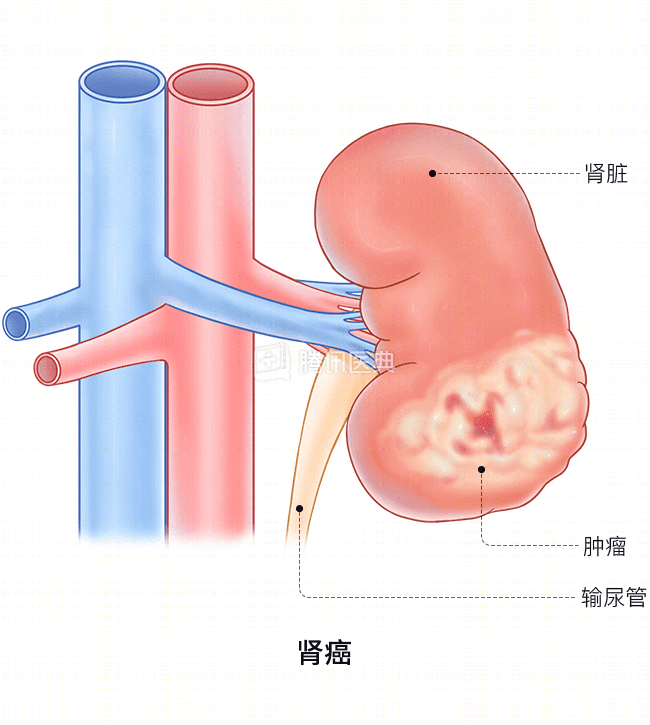
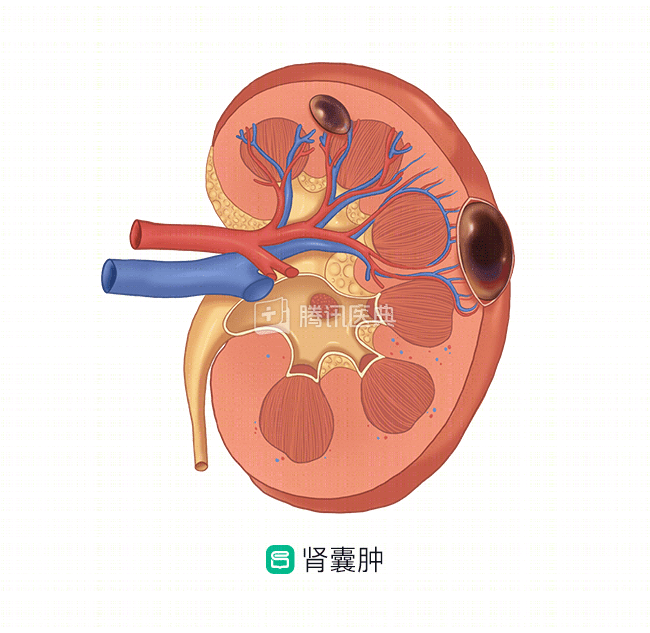
| Characteristics | Kidney cancer is a malignant tumor. | Renal cysts are the most common cystic lesions of the adult kidney, either solitary or multiple, unilateral or bilateral, and can be tens of centimeters large or a few millimeters small |
| Etiology | The etiology is unclear, with smoking in men being a widely recognized cause, and several other factors such as aflatoxins, viruses, and radiation may also cause it. | The current etiology is unclear and may be associated with congenital dysplasia, genetic mutations, infections, and toxins. |
| Clinical presentation |
The triad of “pain, hematuria, and lump in the lower back” is now rare in kidney cancer. The wall of the kidney cancer capsule is irregular on ultrasound and CT, and the capsule has tumor-like contents with enhancement. There are usually no obvious clinical symptoms and it is often detected by chance. It causes symptoms when the kidney cyst grows to a certain size, has intracapsular hemorrhage, secondary infection, or compression of adjacent renal parenchyma. Common symptoms are pain in the lateral abdomen or back and microscopic hematuria.
|
|
| Treatment |
The treatment plan and prognosis of kidney cancer are based on the stage of the tumor, commonly known as Robson stage and TNM stage. The treatment of kidney cancer still relies mainly on surgery, which can be divided into radical surgery and kidney unit-preserving surgery depending on the tumor; Radiotherapy and chemotherapy can be used as palliative treatment to relieve pain and prolong life; Targeted drug therapy based on genetic testing is now a new hot topic. |
Cysts <4 cm in diameter, no significant compression of the pelvis or calyces, no infection, malignancy, hypertension, or no significant symptoms require only close follow-up and regular ultrasound review. Simple renal cysts ≥4 cm can be managed accordingly, and there are currently two main treatment modalities:
|
After clarifying the characteristics of kidney cancer and cysts, the most important thing to do is to get a “plain + enhanced thin-section CT scan” to determine whether the cyst is simple or complex.
- If the cyst is simple, not large and does not affect renal function, it can be observed regularly (annual ultrasound). If the cyst is large and may affect renal function, and if your health condition allows, laparoscopic renal cyst debulking is recommended, and the removed cyst wall can be sent for pathological examination to clarify its nature.
- If the cyst is complex, then it should be treated more carefully and surgical treatment is recommended to remove the cystic lesion intact for examination, rather than simply performing a puncture or debulking procedure.
- If the cyst is small and cannot be determined with certainty at this time, outpatient follow-up with regular ultrasound and CT for close observation is recommended, rather than hasty management.